Anti-double stranded DNA (Anti-dsDNA) antibodies are a group of anti-nuclear antibodies (ANA) the target antigen of which is double stranded DNA. Blood tests such as enzyme-linked immunosorbent assay (ELISA) and immunofluorescence are routinely performed to detect anti-dsDNA antibodies in diagnostic laboratories. They are highly diagnostic of systemic lupus erythematosus (SLE) and are implicated in the pathogenesis of lupus nephritis.[1][2]
Discovery
The first evidence for antinuclear antibodies arose in 1948 when Hargraves, Richmond and Morton discovered the LE cell.[3] These abnormal cells, which are found in the bone marrow of persons who have SLE are categorised as polymorphonuclear leukocytes with phagocytosed whole nuclei.[4] Subsequently, in 1957, antibodies to dsDNA were the first autoantibodies to be identified in patients with SLE.[5]
Antibody production
Although the exact mechanism of the generation of dsDNA antibodies is still unknown, it is likely that extracellular DNA is one cause of an immune response against dsDNA. There is a great deal of evidence supporting the idea that dead or dying cells are one major source of this extracellular DNA.[6] Apoptosis is the highly organised process of programmed cell death in which the cell degrades the nuclear DNA and signals for phagocytosis. In people with SLE and other autoimmune disorders this process is thought to be defective, causing either an increase in cell death and/or a decrease in the rate of dead cell clearance.[7]
There is a higher rate of apoptosis in people with SLE and various changes in genes and proteins have been implicated in the defects in apoptosis. These include increased levels of soluble Fas and bcl-2 and polymorphisms in the programmed cell death 1 and runt-related transcription factor X1.[7]
Blebs on apoptotic cells contain nearly all the autoantigens found in SLE, and phagocytes bind these apoptotic cells and phagocytose them. If this process is defective, these autoantigens can be released into the circulation allowing an immune response. Serum amyloid P component is a protein that is thought to aid in the clearance of chromatin produced by apoptotic cells and deficiencies in this protein have been shown (in mice) to cause spontaneous formation of ANA. Autoantigens present on the blebs of apoptotic cells are also prone to modification, which can increase their immunogenicity.[7][8]
Upon release of nuclear proteins and chromatin, antigen presenting cells, such as dendritic cells and macrophages, display these antigens to T helper cells. Although the details of this process are still controversial, evidence shows that to produce an immune response, DNA must activate an antigen presenting cell to produce type 1 interferons. This cytokine serves to induce maturation of plasmacytoid dendritic cells (PDCs) so that they can display their antigens to T helper cells. The mechanism in which eukaryotic DNA activates these cells is still as yet unclear; however, immunogenic CpG sequences have been found to either activate PDCs or act as adjuvant in the response to eukaryotic DNA. CpG motif DNA acts via the pattern recognition receptor, toll-like receptor 9, found highly expressed in PDCs and B cells. The T helper cells then activate B cells, which are also in the presence of these antigens, causing the production of autoantibodies.[6][9][10][11]
Anti-dsDNA antibodies can also be produced through infection via a mechanism known as molecular mimicry. Upon exposure to pneumococcal polysaccharides, cross reactive antibodies between dsDNA and pneumococcal polysaccharides are produced in lupus.[12] Epstein–Barr virus is also known to induce dsDNA antibodies, as seen after immunisation of animals with EBNA-1 epitopes.[13]
Anti-dsDNA antibodies might also be created secondary to the production of antibodies to other proteins within the nucleosome. Mice that have T cells directed towards the nucleosome can elicit a response to other antigens such as dsDNA and histone via a mechanism known as antigen spreading. This effect can also occur after an infection causes the production of autoantibodies to other structures within the nucleus.[13][14]
Role in disease
SLE
Anti-dsDNA antibodies are incredibly specific for SLE, with studies quoting nearly 100%, and are therefore used in the diagnosis of SLE. Higher titres of anti-dsDNA antibodies are more suggestive of SLE and lower titres can be found in people without the disease. In contrast to the high specificity, estimates of 25–85% have been observed for the sensitivity of anti-dsDNA in SLE. Therefore, presence of anti-dsDNA antibodies are suggestive of SLE, however an absence of the antibodies does not rule out the disease.[1]
The levels of circulating anti-dsDNA antibodies fluctuate with disease activity in SLE. Increases in titres of the antibodies can coincide with, or even precede an increase of disease activity. For this reason titres are serially monitored by clinicians to assess disease progression. Titres are monitored more often in cases of more active lupus than that of less active lupus at intervals of 1–3 months and 6–12 months, respectively.[1]
Anti-dsDNA antibodies are highly associated with glomerulonephritis in SLE, although some patients with high titers of anti-dsDNA antibodies do not develop renal disease. This is most likely due to the fact that anti-dsDNA are a heterogeneous population, some of which have been found not to be pathogenic. Anti-dsDNA antibodies can be present in normal individuals, however these antibodies are usually low avidity IgM isotype. In contrast, pathogenic anti-dsDNA antibodies found in SLE are usually of IgG isotype and show high avidity for dsDNA.[15] One possible mechanism for anti-dsDNA and their role in nephritis is the formation of immune complexes that arise by indirect binding to DNA or nucleosomes that are adhered to the glomerular basement membrane (GBM). Another mechanism is direct binding of antibodies to GBM antigens such as C1q, nucleosomal proteins, heparin sulphate or laminin, which can initiate an inflammatory response by activating complement. They can also be internalised by certain molecules on the GBM cells and cause inflammatory cascades, proliferation and alteration of cellular functions.[2][16][17]
Rheumatoid arthritis
Patients with rheumatoid arthritis can develop anti-dsDNA antibodies, however they are usually treatment related. Anti-TNFα biological therapies, such as adalimumab, infliximab and etanercept, can often induce the production of anti-dsDNA antibodies. They are usually low avidity and are only detectable transiently after treatment. The presence of these antibodies can induce a lupus-like syndrome in some cases.[18][19]
Viral infection
Infection with viral pathogens can induce anti-dsDNA antibodies transiently. Human immunodeficiency virus, parvovirus B19 and BK virus are known to induce these antibodies.[20][21]
Other diseases
There is little evidence supporting the association between anti-dsDNA antibodies and other diseases. Occasionally the monoclonal proteins produced by myeloma patients can be anti-dsDNA. Also, some patients with type 1 autoimmune hepatitis produce anti-dsDNA antibodies.[22][23]
Detection and quantitation
A variety of assay formats can be used to detect and quantify anti-dsDNA antibodies but there is no 'gold standard' for diagnostic purposes and the concordance between different assays/methods is low.[24]
Farr assay
The Farr assay is used to quantify the amount of anti-dsDNA antibodies in serum. Ammonium sulphate is used to precipitate antigen-antibody complexes that form if the sera contains antibodies to dsDNA. The quantity of these antibodies is determined by using radioactively labelled dsDNA. Although this test is very specific, it is of little use in routine diagnostic laboratories due to its laboriousness and use of radioactive materials. The Farr assay is one of the only tests available that detects high avidity antibodies (along with Crithidia luciliae) and also has the ability to detect antibodies of any isotype.[15]
PEG
The polyethylene glycol (PEG) assay precipitates DNA-antibody complexes, similar to the Farr Assay. However, unlike the Farr Assay it does not dissociate the low avidity antibody complexes, allowing for the detection of both high and low avidity anti-dsDNA antibodies.[25]
Immunofluorescence
Animal Tissue
Animal tissue was the first substrate for immunofluorescent detection of antinuclear antibodies and has been in use since the late 1950s. Liver and kidney tissue sections from animals such as rats are used to identify anti-dsDNA antibodies. This substrate has largely been superseded by the use of HEp-2 cells.[1]
HEp-2
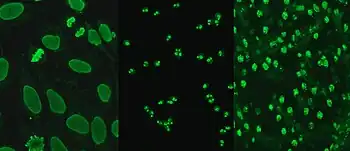
Hep-2 cells, originally of laryngeal carcinoma origin, are actually a contamination of HeLa cells.[26] They are routinely used in the diagnosis of ANA in diagnostic laboratories. HEp-2 cells provide a greater ability to differentiate patterns of ANA than animal sections, due to the large nuclei and high mitotic rate of the cell line. Upon incubation with serum containing anti-dsDNA antibodies and fluorescent labelled secondary antibodies, homogeneous staining of interphase nuclei and condensed chromosomal staining of mitotic cells can be seen.[27]
Crithidia
Crithidia luciliae is a haemoflagellate protist with an organelle known as the kinetoplast. This organelle contains a high concentration of circular DNA with no recognisable nuclear antigens, allowing for the reliable detection of anti-dsDNA antibodies. The kinetoplast fluoresces if serum contains high avidity anti-dsDNA antibodies. This test has a higher specificity than EIA because it uses unprocessed DNA. Processed DNA can contain regions of ssDNA, allowing detection of anti-ssDNA antibodies, which can give false positive results.[1][28]
EIA
EIA (enzyme immunoassay) detects antibodies using a DNA-coated polystyrene microtitre plate. The DNA used in these assays is often recombinant dsDNA or from calf thymus extract.[29] Upon incubation with serum containing anti-dsDNA antibodies, the antibodies will bind to the DNA and can then be visualised using enzyme-linked secondary antibodies. This assay can be quantitative or semi-quantitative, allowing for estimations of the levels of anti-dsDNA antibodies. This test can produce false positives due to contamination of ssDNA from denatured dsDNA. EIA detects low and high avidity anti-dsDNA antibodies, increasing its sensitivity and reducing its specificity.[1]
Flow cytometry
Flow cytometry for the detection of ANA uses multiplexed polystyrene beads coated with multiple autoantigens, such as SSA, SSB, Sm, RNP, Scl-70, Jo-1, dsDNA, centromere B and histone. Serum is incubated with the beads and in the presence of anti-dsDNA antibodies, or any other ANA, the antibodies will bind and fluorescent labelled secondary antibodies will be used for detection. The beads are run through a flow cell which uses a laser to detect fluorescence.[30][31]
Multiplex immunoassay (MIA)
Similar to the flow cytometry method of ANA detection, the MIA uses wells containing autoantigens and HEp-2 extract coated beads. The bead sets are coated with specific autoantigens and can be detected individually to allow identification of the particular autoantibody. Automated analysis of the well fluorescence allows for rapid detection of autoantibodies.[30][32]
Microarrays
Microarrays are a newly emerging method for the detection of ANA. Individual autoantigens are deposited in an array of dots onto a surface such as polystyrene. A single array could consist of hundreds of autoantigens for screening of multiple autoimmune diseases simultaneously. If anti-dsDNA antibodies are present, incubation of serum and the microarray allow for binding and the dots can then be visualised using a fluorescent labelled anti-IgG antibody.[33]
Therapeutics
As a result of the highly specific nature of antibodies, they can be engineered to target and bind key motifs. These motifs can be key features within the pathogenesis of particular diseases, for example human papillomavirus.[34]
References
- 1 2 3 4 5 6 Kavanaugh A, Tomar R, Reveille J, Solomon DH, Homburger HA (January 2000). "Guidelines for clinical use of the antinuclear antibody test and tests for specific autoantibodies to nuclear antigens. American College of Pathologists". Arch. Pathol. Lab. Med. 124 (1): 71–81. doi:10.5858/2000-124-0071-GFCUOT. PMID 10629135.
- 1 2 Mortensen ES, Fenton KA, Rekvig OP (February 2008). "Lupus nephritis: the central role of nucleosomes revealed". Am. J. Pathol. 172 (2): 275–83. doi:10.2353/ajpath.2008.070563. PMC 2312358. PMID 18187568.
- ↑ Hargraves MM, Richmond H, Morton R (January 1948). "Presentation of two bone marrow elements; the tart cell and the L.E. cell". Proceedings of the Staff Meetings of the Mayo Clinic. 23 (2): 25–8. PMID 18921142.
- ↑ Shao WH, Cohen PL (2011). "Disturbances of apoptotic cell clearance in systemic lupus erythematosus". Arthritis Research & Therapy. 13 (1): 202. doi:10.1186/ar3206. PMC 3157636. PMID 21371352.
- ↑ Stollar BD (1989). "Immunochemistry of DNA". International Reviews of Immunology. 5 (1): 1–22. doi:10.3109/08830188909086987. PMID 2491157.
- 1 2 Su KY, Pisetsky DS (September 2009). "The role of extracellular DNA in autoimmunity in SLE". Scand. J. Immunol. 70 (3): 175–83. doi:10.1111/j.1365-3083.2009.02300.x. PMID 19703007. S2CID 205382203.
- 1 2 3 Dieker JW, van der Vlag J, Berden JH (February 2004). "Deranged removal of apoptotic cells: its role in the genesis of lupus". Nephrol. Dial. Transplant. 19 (2): 282–5. doi:10.1093/ndt/gfg485. hdl:2066/58078. PMID 14736945.
- ↑ Smeenk RJ (June 2000). "Antinuclear antibodies: cause of disease or caused by disease?". Rheumatology (Oxford). 39 (6): 581–4. doi:10.1093/rheumatology/39.6.581. PMID 10888701.
- ↑ Graham KL, Utz PJ (September 2005). "Sources of autoantigens in systemic lupus erythematosus". Current Opinion in Rheumatology. 17 (5): 513–7. doi:10.1097/01.bor.0000171215.87993.6b. PMID 16093826. S2CID 18465332.
- ↑ Marshak-Rothstein A (November 2006). "Toll-like receptors in systemic autoimmune disease". Nature Reviews Immunology. 6 (11): 823–35. doi:10.1038/nri1957. PMC 7097510. PMID 17063184.
- ↑ Rekvig OP, Nossent JC (February 2003). "Anti-double-stranded DNA antibodies, nucleosomes, and systemic lupus erythematosus: a time for new paradigms?". Arthritis Rheum. 48 (2): 300–12. doi:10.1002/art.10739. PMID 12571837.
- ↑ Blank M, Barzilai O, Shoenfeld Y (February 2007). "Molecular mimicry and auto-immunity". Clin Rev Allergy Immunol. 32 (1): 111–8. doi:10.1007/bf02686087. PMID 17426366. S2CID 20475334.
- 1 2 Poole BD, Scofield RH, Harley JB, James JA (February 2006). "Epstein-Barr virus and molecular mimicry in systemic lupus erythematosus". Autoimmunity. 39 (1): 63–70. doi:10.1080/08916930500484849. PMID 16455583. S2CID 9844130.
- ↑ Berden JH (August 2003). "Lupus nephritis: consequence of disturbed removal of apoptotic cells?". Neth J Med. 61 (8): 233–8. PMID 14628957.
- 1 2 Egner W (June 2000). "The use of laboratory tests in the diagnosis of SLE". J. Clin. Pathol. 53 (6): 424–32. doi:10.1136/jcp.53.6.424. PMC 1731203. PMID 10911799.
- ↑ Mok CC, Lau CS (July 2003). "Pathogenesis of systemic lupus erythematosus". J. Clin. Pathol. 56 (7): 481–90. doi:10.1136/jcp.56.7.481. PMC 1769989. PMID 12835292.
- ↑ Yung S, Chan TM (February 2008). "Anti-DNA antibodies in the pathogenesis of lupus nephritis--the emerging mechanisms". Autoimmun Rev. 7 (4): 317–21. doi:10.1016/j.autrev.2007.12.001. PMID 18295737.
- ↑ Hanauer SB (September 1999). "Review article: safety of infliximab in clinical trials". Aliment. Pharmacol. Ther. 13 (Suppl 4): 16–22, discussion 38. doi:10.1046/j.1365-2036.1999.00027.x. PMID 10597335. S2CID 1642477.
- ↑ Hyrich KL, Silman AJ, Watson KD, Symmons DP (December 2004). "Anti-tumour necrosis factor alpha therapy in rheumatoid arthritis: an update on safety". Ann. Rheum. Dis. 63 (12): 1538–43. doi:10.1136/ard.2004.024737. PMC 1754871. PMID 15242866.
- ↑ Hansen KE, Arnason J, Bridges AJ (April 1998). "Autoantibodies and common viral illnesses". Semin. Arthritis Rheum. 27 (5): 263–71. doi:10.1016/s0049-0172(98)80047-4. PMID 9572708.
- ↑ Reploeg MD, Storch GA, Clifford DB (July 2001). "Bk virus: a clinical review". Clin. Infect. Dis. 33 (2): 191–202. doi:10.1086/321813. PMID 11418879.
- ↑ Isenberg DA, Manson JJ, Ehrenstein MR, Rahman A (July 2007). "Fifty years of anti-ds DNA antibodies: are we approaching journey's end?". Rheumatology (Oxford). 46 (7): 1052–6. doi:10.1093/rheumatology/kem112. PMID 17500073.
- ↑ Maya R, Gershwin ME, Shoenfeld Y (February 2008). "Hepatitis B virus (HBV) and autoimmune disease". Clin Rev Allergy Immunol. 34 (1): 85–102. doi:10.1007/s12016-007-8013-6. PMID 18270862. S2CID 9324159.
- ↑ Enocsson H; Sjöwall C; Wirestam L; Dahle C; Kastbom A; Rönnelid J; Wetterö J; Skogh T (2015). "Four Anti-dsDNA Antibody Assays in Relation to Systemic Lupus Erythematosus Disease Specificity and Activity". J Rheumatol. 42 (5): 817–25. doi:10.3899/jrheum.140677. PMID 25684763. S2CID 207570256.
- ↑ Nossent JC, Huysen V, Smeenk RJ, Swaak AJ (September 1989). "Low avidity antibodies to dsDNA as a diagnostic tool". Ann. Rheum. Dis. 48 (9): 748–52. doi:10.1136/ard.48.9.748. PMC 1003868. PMID 2802796.
- ↑ Lacroix M (January 2008). "Persistent use of "false" cell lines". Int. J. Cancer. 122 (1): 1–4. doi:10.1002/ijc.23233. PMID 17960586. S2CID 27432788.
- ↑ Bradwell, A. R. (2003). Atlas of HEp-2 patterns and laboratory techniques. Birmingham: Binding Site. ISBN 0-7044-2437-1.
- ↑ Slater NG, Cameron JS, Lessof MH (September 1976). "The Crithidia luciliae kinetoplast immunofluorescence test in systemic lupus erythematosus". Clin. Exp. Immunol. 25 (3): 480–6. PMC 1541410. PMID 786521.
- ↑ Burnett, David; Crocker, John R. (1999). The Science of Laboratory Diagnosis. ISIS Medical Media. pp. 494–495. ISBN 1-899066-62-4.
- 1 2 Yu X, Schneiderhan-Marra N, Joos TO (2011). "[Protein microarrays and personalized medicine]". Ann. Biol. Clin. (Paris) (in French). 69 (1): 17–29. doi:10.1684/abc.2010.0512. PMID 21463992.
- ↑ Avaniss-Aghajani E, Berzon S, Sarkissian A (May 2007). "Clinical value of multiplexed bead-based immunoassays for detection of autoantibodies to nuclear antigens". Clin. Vaccine Immunol. 14 (5): 505–9. doi:10.1128/CVI.00034-07. PMC 1865627. PMID 17376860.
- ↑ Kumar Y, Bhatia A, Minz RW (2009). "Antinuclear antibodies and their detection methods in diagnosis of connective tissue diseases: a journey revisited". Diagn Pathol. 4: 1. doi:10.1186/1746-1596-4-1. PMC 2628865. PMID 19121207.
- ↑ Hueber W, Utz PJ, Steinman L, Robinson WH (2002). "Autoantibody profiling for the study and treatment of autoimmune disease". Arthritis Res. 4 (5): 290–5. doi:10.1186/ar426. PMC 128938. PMID 12223102.
- ↑ Cerutti ML, Centeno JM, Goldbaum FA, de Prat-Gay G (2001). "Generation of Sequence-specific, High Affinity Anti-DNA Antibodies". Journal of Biological Chemistry. 276 (16): 12766–12773. doi:10.1074/jbc.M100260200. hdl:11336/48130. PMID 11279040. S2CID 26068816.