| Cervicocranial syndrome | |
|---|---|
| Other names | Craniocervical Junction Syndrome |
| Specialty | Neurology |
Cervicocranial syndrome or (Craniocervical Junction Syndrome: CCJ syndrome) is a neurological illness. It is a combination of symptoms that are caused by an abnormality in the neck. The bones of the neck that are affected are cervical vertebrae (C1 - C7). This syndrome can be identified by confirming cervical bone shifts, collapsed cervical bones or misalignment of the cervical bone leading to improper functioning of cervical spinal nerves.Greenberg Regenerative Medicine | Bryn Mawr, Pennsylvania Cervicocranial syndrome is either congenital or acquired (as a result of injury or disease). Some examples of diseases that could result in cervicocranial syndrome are Chiari disease, Klippel-Feil malformation[1] osteoarthritis, and trauma.[2] Treatment options include neck braces, pain medication and surgery. The quality of life for individuals suffering from CCJ syndrome can improve through surgery.[3]

Signs and Symptoms
Cervicocranial syndrome has a wide range of symptoms. These symptoms[4] often include:
- Vertigo
- Chronic Headache aka Cephalea
- Tinnitus[4]
- Facial Pain[5]
- Ear Pain
- Dysphagia
- Carotidynia
- Neck Pain (ex: during movement such extension and flexion)[5]
- Syncope[6]
- Sinus congestion
- Neck Crepitus Sound
- Loss of vision
- Involuntary eye-movement
- Severe Fatigue
- Chest Pain
- Brain Fog
Cause
The cause of cervicocranial syndrome is either due to a defect (genetic mutation or development of diseases later in life) or an injury pertaining to the neck: cervical area, that damages the spinal nerves traveling through the cervical region[7][5] resulting in ventral subluxation.[8] Examples of cases that can result in cervicocranial syndrome are: car accidents, trauma, osteoarthritis, tumor, degenerative pathology[6] and other numerous causes of vertebral instability. There is no single cause that can mainly cause cervicocranial syndrome.
Genetic

The genes GDF6, GDF3, MEOX1 used as examples, encode for making proteins that help with development. For example GDF6 gene plays an important role in bone development and joint formation.[9] The mutation in these genes can result in Klippel-Feil syndrome. As a result of having congenital Klippel-Feil syndrome, the spinal anatomy of the individual will present abnormal fusion of any two of the seven cervical bones in the neck.[10] This is considered to be an anomaly of cervical bones.[11] It affects the functioning of cervical spinal nerves (C1 - C8) because of compression on the spinal cord. Spinal stenosis also adds damage to the spinal cord resulting in symptoms that are caused by cervicocranial syndrome.[12]
Trauma
Traumatic injuries are caused when external forces damage the cervical spine, giving rise to various symptoms.[13] In a motor vehicle accident, the vehicle jerks the neck forward and backward resulting in cervical spine damage. This is called whiplash.[14] The neurological and biological symptoms resulting from neck trauma emerge as a culmination of clinically isolated or combined symptoms caused by cervicocranial syndrome.[13]
Pathophysiology
The body is innervated by spinal nerves that branch off from the spinal cord.[15] This innervation enables the brain to receive sensory inputs and send motor outputs. There are 8 cervical spinal nerves of the peripheral nervous system. Cervical spinal nerves C1, C2 and C3 help control the movements of the head and neck. Cervical spinal nerve C4 helps control upward shoulder movements. Cervical spinal nerve C3, C4 and C5 help power the diaphragm and aid in breathing. Cervical spinal nerve C6 helps in wrist extension and some functioning of biceps. Cervical spinal nerve C7 controls triceps and wrist extension. Cervical spinal nerve C8 helps control the hand.[15] The cervicocranial syndrome occurs when symptoms arise due to cervical vertebrae damage (misalignment, collapse, shift or disease, such as tumor) resulting in the improper functioning of the cervical spinal nerves.
Examples of Cervicocranial Syndrome Pathophysiology
Chordoma
The craniocervical junction region comprises C1 (Atlas), C2 (Axis) and the lower part of the skull: occipital bone. In case of tumor: chordoma, in the craniocervical junction region, this leads to pressure on the cervical spinal nerves, which results in their improper functioning of the cervical spinal nerves. Hence, leading to symptoms of cervicocranial syndrome.[16] To decompress the pressure on the nerves, the tumor is removed and the foramen through which the spinal nerve roots travel through is enlarged to allow the nerves to pass through so that symptoms of cervicocranial syndrome can be reduced and the nerves are sending signals.
Atlanto-Occipital Assimilation
When the occipital bone and the atlas (C1) are fused together in a condition called atlanto-occipital assimilation, it causes improper functioning of the cervical spinal nerves due to the vascular compression. Surgical procedure can decompress the nerves and reduce symptoms.[17][18][19]
Trauma
Traumatic injuries are caused when external forces damage the cervical spine, giving rise to various symptoms.[13] In a car accident, the vehicle jerks the neck forward and backward resulting in cervical spine damage resulting in a whiplash. As a result, the cervical spine become misaligned and produces direct spinal cord irritation creating tighter muscles on one side of the body[20] Neck braces can help temporarily. Surgery is required if needed. Non-surgical treatment, to realign spinal misalignment, is corrected by a chiropractor.
Diagnosis
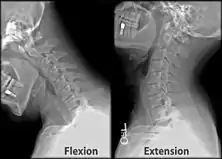
Once there is an onset of the symptoms in the patient, the patients are screened through cervical-spinal imaging techniques: X-ray, CT, MRI. The scanning technique points out any cervical vertebrae defects and misalignments. (Image 1. and 2.) When cervicocranial syndrome is caused as a result of a genetic disease, then family history and genetic testing aid in making an accurate diagnosis of cervicocranial syndrome.

Prevention/Treatment
The treatment options vary since there are numerous causes of cervicocranial syndrome. General treatments include:
- Pressure release via realignment of the vertebrae
- Pain medication: acetominophen, aspirin, or ibuprofen
- Manipulation of neck by Chiropractor : For example, vertigo symptoms can be relieved[21]
- Neck braces to avoid movement of neck and provide stability
- Physical therapy
- Injection: Combination (anesthetic and cortisone) drug to help alleviate the pain
- Surgery to restore function and form of the spine
- Cervical spinal cord stimulation (cSCS) [22]
When cervicocranial syndrome is caused by a mutation in genes and it runs in the family due to other co-morbidities, genetic counseling helps patients cover risks, prevention and expectations of caring and passing genes to a newborn.[23]
Prognosis
The prognosis of an individual living with cervicocranial syndrome varies because of the multiple causes such as co-morbidities and varied trauma. Instability of the cervical spine can cause endangerment of patients and their neurological integrity.[24] Correction and decompression cervical spinal surgeries significantly increase quality of life and reduce symptoms. Post-surgery, 93 to 100 percent patients report reduced cervicocranial syndrome symptoms such as neck pain.[25][26]
Epidemiology
Cervicocranial syndrome significantly affects the aging world population and is associated with significant morbidity.[26] It affects men and women equally when occurring due to atlanto-occipital assimilation.[27] Increased incidences among low-socioeconomic groups and among groups that do not have access to healthcare show subsequently higher rates of morbidity and mortality.[26]
Research Directions
Cervicocranial syndrome can be caused with or as a result of numerous neurological problems so not one single disease can be pinpointed. Further research can explore the common neurological problems causing cervicocranial syndrome and look at various treatments including therapeutic ones.
For example, a study, "The influence of cranio-cervical rehabilitation in patients with myofascial temporomandibular pain disorders," [28] explored the therapeutic options of physical therapy and concluded that 88% from a total of 98 patients (79 female and 19 male), felt reduced pain. On the contrary another study, "The efficacy of manual therapy and therapeutic exercise in patients with chronic neck pain: A narrative review" [29] conducted in 2018, concluded that there is a lack of evidence that support therapeutic exercise to reduce neck pain via manipulation.
References
- ↑ Avellaneda Fernández, Alfredo; Isla Guerrero, Alberto; Izquierdo Martínez, Maravillas; Amado Vázquez, María Eugenia; Barrón Fernández, Javier; Chesa i Octavio, Ester; De la Cruz Labrado, Javier; Escribano Silva, Mercedes; Fernández de Gamboa Fernández de Araoz, Marta; García-Ramos, Rocío; García Ribes, Miguel (2009-12-17). "Malformations of the craniocervical junction (chiari type I and syringomyelia: classification, diagnosis and treatment)". BMC Musculoskeletal Disorders. 10 (1): S1. doi:10.1186/1471-2474-10-S1-S1. ISSN 1471-2474. PMC 2796052. PMID 20018097.
- ↑ Smoker, Wendy R. K.; Khanna, Geetika (October 2008). "Imaging the craniocervical junction". Child's Nervous System. 24 (10): 1123–1145. doi:10.1007/s00381-008-0601-0. ISSN 0256-7040. PMID 18461336. S2CID 9127674.
- ↑ Henderson, Fraser C.; Francomano, C. A.; Koby, M.; Tuchman, K.; Adcock, J.; Patel, S. (2019). "Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization". Neurosurgical Review. 42 (4): 915–936. doi:10.1007/s10143-018-01070-4. ISSN 0344-5607. PMC 6821667. PMID 30627832.
- 1 2 Terrahe, K. (June 1985). "[The cervico-cranial syndrome in the practice of the otorhinolaryngologist]". Laryngologie, Rhinologie, Otologie. 64 (6): 292–299. ISSN 0340-1588. PMID 4033308.
- 1 2 3 "Cervicocranial syndrome (Concept Id: C2355645) - MedGen - NCBI". www.ncbi.nlm.nih.gov. Retrieved 2020-11-11.
- 1 2 Cornelius, Jan Frederick; Pop, Raoul; Fricia, Marco; George, Bernard; Chibbaro, Salvatore (2019). "Compression Syndromes of the Vertebral Artery at the Craniocervical Junction". New Trends in Craniovertebral Junction Surgery. Acta Neurochirurgica Supplement. Vol. 125. pp. 151–158. doi:10.1007/978-3-319-62515-7_22. ISBN 978-3-319-62514-0. ISSN 0065-1419. PMID 30610316. S2CID 58545984.
- ↑ "Cervicocranial syndrome (Concept Id: C2355645) - MedGen - NCBI". www.ncbi.nlm.nih.gov. Retrieved 2020-11-11.
- ↑ Vesela, Martina; Stetkarova, Ivana; Lisy, Jiri (November 2005). "Prevalence of C1/C2 involvement in Czech rheumatoid arthritis patients, correlation of pain intensity, and distance of ventral subluxation". Rheumatology International. 26 (1): 12–15. doi:10.1007/s00296-004-0506-5. ISSN 0172-8172. PMID 15666164. S2CID 9617977.
- ↑ Mohamed, Jawahir Y.; Faqeih, Eissa; Alsiddiky, Abdulmonem; Alshammari, Muneera J.; Ibrahim, Niema A.; Alkuraya, Fowzan S. (2013-01-10). "Mutations in MEOX1, Encoding Mesenchyme Homeobox 1, Cause Klippel-Feil Anomaly". The American Journal of Human Genetics. 92 (1): 157–161. doi:10.1016/j.ajhg.2012.11.016. ISSN 0002-9297. PMC 3542464. PMID 23290072.
- ↑ Kaplan, Kevin M.; Spivak, Jeffrey M.; Bendo, John A. (2005-09-01). "Embryology of the spine and associated congenital abnormalities". The Spine Journal. 5 (5): 564–576. doi:10.1016/j.spinee.2004.10.044. ISSN 1529-9430. PMID 16153587.
- ↑ "Congenital Osseous Anomalies of the Upper and Lower... : JBJS". LWW. Retrieved 2020-12-17.
- ↑ "The Influence of Spinal Canal Narrowing and Timing of... : Spine". LWW. Retrieved 2020-12-17.
- 1 2 3 Tanaka, Nobuhiro; Atesok, Kivanc; Nakanishi, Kazuyoshi; Kamei, Naosuke; Nakamae, Toshio; Kotaka, Shinji; Adachi, Nobuo (2018-02-28). "Pathology and Treatment of Traumatic Cervical Spine Syndrome: Whiplash Injury". Advances in Orthopedics. 2018: 1–6. doi:10.1155/2018/4765050. ISSN 2090-3464. PMC 5851023. PMID 29682354.
- ↑ Panjabi, Manohar M.; Cholewicki, Jacek; Nibu, Kimio; Grauer, Jonathan N.; Babat, Lawrence B.; Dvorak, Jiri (1998-06-01). "Mechanism of whiplash injury". Clinical Biomechanics. 13 (4): 239–249. doi:10.1016/S0268-0033(98)00033-3. ISSN 0268-0033. PMID 11415793.
- 1 2 Waxenbaum, Joshua A.; Reddy, Vamsi; Bordoni, Bruno (2020), "Anatomy, Head and Neck, Cervical Nerves", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30844163, retrieved 2020-12-17
- ↑ Kratimenos, George P.; Crockard, H. Alan (1993-01-01). "The far lateral approach for ventrally placed foramen magnum and upper cervical spine tumours". British Journal of Neurosurgery. 7 (2): 129–140. doi:10.3109/02688699309103469. ISSN 0268-8697. PMID 8494614.
- ↑ Rubin, Michael (January 2022). "Craniocervical Junction Disorders - Brain, Spinal Cord, and Nerve Disorders". Merck Manual Consumer Version. Retrieved 2022-09-09.
- ↑ Menezes, Arnold H. (1997-09-01). "Craniovertebral junction anomalies: Diagnosis and management". Seminars in Pediatric Neurology. Neurosurgical Issues for the Pediatric Patient. 4 (3): 209–223. doi:10.1016/S1071-9091(97)80038-1. ISSN 1071-9091. PMID 9323790.
- ↑ Iwata, Atsushi; Murata, Miho; Nukina, Nobuyuki; Kanazawa, Ichiro (1998-02-05). "Foramen magnum syndrome caused by atlanto-occipital assimilation". Journal of the Neurological Sciences. 154 (2): 229–231. doi:10.1016/S0022-510X(97)00224-4. ISSN 0022-510X. PMID 9562315.
- ↑ "Society of Chiropractic Orthospinology - An Upper Cervical Procedure - What Is Orthospinology?". orthospinology.org. Retrieved 2020-12-17.
- ↑ Mahlstedt, K.; Westhofen, M.; König, K. (May 1992). "[Therapy of functional disorders of the craniovertebral joints in vestibular diseases]". Laryngo- Rhino- Otologie. 71 (5): 246–250. doi:10.1055/s-2007-997289. ISSN 0935-8943. PMID 1616544. S2CID 72840124.
- ↑ Chan, Andrew K.; Winkler, Ethan A.; Jacques, Line (2016-07-01). "Rate of perioperative neurological complications after surgery for cervical spinal cord stimulation". Journal of Neurosurgery: Spine. 25 (1): 31–38. doi:10.3171/2015.10.SPINE15670. PMID 26943257.
- ↑ Rossi, Ernest L.; Cozzolino, Mauro; Mortimer, Jane; Atkinson, David; Rossi, Kathryn Lane (October 2011). "A Brief Protocol for the Creative Psychosocial Genomic Healing Experience: The 4-Stage Creative Process in Therapeutic Hypnosis and Brief Psychotherapy". American Journal of Clinical Hypnosis. 54 (2): 133–152. doi:10.1080/00029157.2011.605967. ISSN 0002-9157. PMID 22125895. S2CID 34260924.
- ↑ Wenning, Katharina E.; Hoffmann, Martin F. (2020-01-09). "Does isolated atlantoaxial fusion result in better clinical outcome compared to occipitocervical fusion?". Journal of Orthopaedic Surgery and Research. 15 (1): 8. doi:10.1186/s13018-019-1525-y. ISSN 1749-799X. PMC 6953136. PMID 31918713.
- ↑ Yin, Yi-Heng; Qiao, Guang-Yu; Yu, Xin-Guang (2016-11-01). "Surgical Treatment of Occipitocervical Dislocation with Atlas Assimilation and Klippel-Feil Syndrome Using Occipitalized C1 Lateral Mass and C2 Fixation and Reduction Technique". World Neurosurgery. 95: 46–52. doi:10.1016/j.wneu.2016.07.058. ISSN 1878-8750. PMID 27465418.
- 1 2 3 Waheed, Muhammad Abdul-Aziz; Hasan, Sazid; Tan, Lee A.; Bosco, Aju; Reinas, Rui; Wengel, Paula Valerie ter; Hey, Hwee Weng Dennis; Aleem, Ilyas S. (March 2020). "Cervical spine pathology and treatment: a global overview". Journal of Spine Surgery. 6 (1): 340–350. doi:10.21037/jss.2020.01.12. ISSN 2414-4630. PMC 7154356. PMID 32309671.
- ↑ Knipe, Henry. "Atlanto-occipital assimilation | Radiology Reference Article | Radiopaedia.org". Radiopaedia. Retrieved 2020-12-17.
- ↑ Halmova, K.; Holly, D.; Stanko, P. (2017). "The influence of cranio-cervical rehabilitation in patients with myofascial temporomandibular pain disorders". Bratislavske Lekarske Listy. 118 (11): 710–713. doi:10.4149/BLL_2017_134. ISSN 0006-9248. PMID 29216730.
- ↑ The efficacy of manual therapy and therapeutic exercise in patients with chronic neck pain: A narrative review kheljournal.com