| Lennox–Gastaut syndrome | |
|---|---|
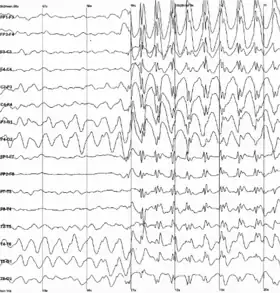 | |
| Generalized 2.5 Hz spike and wave discharges in a child with childhood absence epilepsy | |
| Specialty | Neurology |
Lennox–Gastaut syndrome (LGS) is a complex, rare, and severe childhood-onset epilepsy syndrome. It is characterized by multiple and concurrent seizure types including tonic seizure, cognitive dysfunction, and slow spike waves on electroencephalogram (EEG), which are very abnormal.[1] Typically, it presents in children aged 3–5 years and most of the time persists into adulthood with slight changes in the electroclinical phenotype .[2][3] It has been associated with perinatal injuries, congenital infections, brain malformations, brain tumors, genetic disorders such as tuberous sclerosis and numerous gene mutations. Sometimes LGS is observed after infantile epileptic spasm syndrome (formerly called West syndrome). The prognosis for LGS is marked by a 5% mortality in childhood and persistent seizures into adulthood (at least 90% of adults with LGS still have seizures).[4]
LGS was named for neurologists William G. Lennox (Boston, US) and Henri Gastaut (Marseille, France),[5] who independently described the condition. The international LGS Awareness Day is on November 1.[6]
Signs and symptoms
The symptoms vary and progress with age and are characterized by a triad of seizures including tonic seizure, cognitive dysfunction, and EEG findings. The triad may not fully emerge until 1–2 years after first seizure episode.[1]
Seizures
The peak age of onset of seizures is in the first year of life and the seizures evolve into LGS typically between 3 and 5 years of age.[7] The mainstay symptoms are seizures that are frequent – occurring daily and difficult to treat with anti-seizure medications. An estimated 30% of patients with infantile epileptic spasm syndrome (formerly called West syndrome) have been reported to progress with LGS.[8][9]
Tonic seizures are the most common and present in nearly everyone with LGS.[10][11] They occur most frequently during non-REM sleep (90% of the time). They initially last for a minute or less and are activated by sleep. The presentation can be subtle.[12] They present often as tonic eyelid opening with some changes in breathing coupled with pupillary dilation, urinary incontinence, increased heart rate, and flushing.
Nonconvulsive status epilepticus occurs in about 50% of patients with LGS. The seizures can cause sudden falling often leading to injury. These "drop attacks" are typically the first manifestation of LGS. The attacks are characterized by a single, generalized myoclonic jerk that precedes tonic contraction of axial muscles.
EEG findings
Findings that strongly suggest LGS include abnormal, consistent slow spike-wave (< 3 hertz [Hz]) on awake EEG. The complexes typically consist of a spike (duration < 70 milliseconds) or a sharp wave (70–200 milliseconds), followed first by a positive deep trough, then a negative wave (350–400 milliseconds). Not every wave is preceded by a spike. Bursts increase and decrease without clear onset and offset. Slow spike waves may occur during seizures or between seizures, or may occur in absence of any observable clinical changes. This helps distinguish LGS from the pattern of extended 3-Hz spike-wave discharges.
Causes
The LGS disease pathophysiology is mostly unknown, but some evidence implicates cortical hyperexcitability occurring at critical periods of brain development.
A lot is known about what causes early life seizures and everyone with LGS has it secondary to a seizure etiology. There are two types of LGS etiologies: idiopathic and secondary. The cause of the idiopathic subtype is unknown. The cause of the secondary subtype occurs when an identifiable underlying pathology is responsible and you can see this pathology on an MRI scan. The most common type of LGS (70–78%) is secondary.[13] These patients tend to have a worse prognosis than those with idiopathic LGS.[14] In up to one-third of cases no cause for seizures can be found.[14]
Brain injury
Seizures that then evolve into LGS most often occur secondary to brain damage. The brain damage can occur from perinatal insults, encephalitis, meningitis, tumor, and brain malformation.[1]
Genetic mutations
Other identified causes of early life seizures include genetic disorders such as tuberous sclerosis and inherited deficiency of methylene tetrahydrofolate reductase. Some of these cases once thought to be of unknown cause may have definitive etiology by modern genetic testing.[14]
Progress in genome and exome sequencing is revealing that some individuals diagnosed with Lennox–Gastaut syndrome have de novo mutations in a variety of genes, including CHD2, GABRB3, ALG13 and SCN2A.[15][16] The Epi4K study consortium (2013) observed de novo mutations in at least 15% of a study cohort of 165 patients with LGS and infantile spasms using whole exome sequencing.[17] A 2013 study found a high frequency of rare copy-number variations (CNVs) in adult patients with LGS or LGS-like epilepsy.[18]
Mutations in the IQSEC2 gene have been associated with this syndrome.[19] This gene is located on the short arm of the X chromosome (Xp11.22).
While we know a lot about what causes early life seizures, we do not know why some children's seizures evolve into LGS.
Diagnosis
The diagnosis of LGS should be suspected in children less than 8 years old with seizures of multiple types that cannot be treated with anti-seizure medications. Because of high risk of irreversible brain damage in early stages of syndrome (particularly in infants and young children), early diagnosis is essential. Nobody is born with LGS, it evolves over time, so it may take 1–2 years after first initial seizure for all criteria for diagnosis to emerge, so LGS should be considered if there are suggestive signs and symptoms without presence of complete triad.
To confirm diagnosis, awake and asleep EEG and magnetic resonance imaging (MRI) are performed. MRI is used to detect focal brain lesions.
The diagnosis of LGS should also be considered in adults who have childhood-onset, intractable seizures, and intellectual disability.
Ruling out other diagnoses
Certain diagnoses must be ruled out before diagnosing LGS. These diagnoses are:
- Doose syndrome
- Dravet syndrome
- pseudo-Lennox–Gastaut syndrome (atypical benign partial epilepsy)
LGS is more easily distinguished from Doose syndrome by seizure type after the syndrome has progressed. Doose syndrome has more myoclonic seizures and LGS has more tonic seizures. The Doose syndromes is less likely to have cognitive disabilities.
Pseudo-Lennox–Gastaut syndrome can be distinguished from LGS because pseudo-LGS has different spike-and-wave patterns on EEG.
Treatment
There are several treatment options, including medications, surgery, and diet.
Medications
In most patients with LGS, the treatment does not end seizure recurrence.
The goals of treatment are to lower frequency and severity of seizures to greatest extent possible. There are no studies using only one medication. Lamotrigine and rufinamide used as add-ons are very effective in reducing overall seizures, but do not stop them.[20]
The treatments for LGS has evolved over the years. Various treatments have been shown to have some degree of efficacy. In 1997–1999, lamotrigine was found to be effective and approved by the Food and Drug Administration and Health Canada.[21][22][23] In 1999, topiramate trials showed that topiramate decreased seizure occurrence by more than 50%.[24][25]
Felbamate is the treatment of last resort in the event that everything else fails,[26] and was found to be superior to placebo in controlling treatment resistant partial seizures and atonic seizures.[27][28] However, it has been known to cause aplastic anemia and liver toxicity.[29]
First-line drugs
- valproate (valproic acid, sodium valproate and valproate semisodium)
Second-line drugs
Third-line drugs
- rufinamide[30]
- topiramate[30]
- clobazam [30]
- felbamate[30]
- cannabidiol [31]
Adjuvant drugs
Are the following:
Surgery
In the past, LGS patients were not eligible for surgery, as the medical community thought it to involve the whole brain as a generalized epilepsy in all cases. Since 2010, this assumption has been challenged.[32] Two studies on LGS patients series who underwent curative surgery in Korea[33] and China,[34] showed very good results, up to seizure freedom for 80% of these patients below 5 years old, and 40% above 5 years old. Like all epilepsy curative surgeries, seizures may recur in the years following surgery, but surgery allows the child to have better brain development during the seizure free period.
There are several procedures that have shown efficacy:
- vagus nerve stimulation, which involves implantation of battery-operated generator of intermittent electrical stimuli to an electrode wrapped around left vagus nerve. Some studies have been shown it to have greater than 50% reduction in seizures reported in more than half of patients.
- corpus callosotomy, which has shown to be effective with atonic seizures. This procedure is considered in cases in which vagus nerve stimulation has failed
- transcranial direct current stimulation
- resection
Diet
A ketogenic diet is a diet that causes ketosis, a state in which there is an increased amount of ketones in the body. Adopting and maintaining rigid diet may be difficult for some families. Short-term ketogenic diet might be associated with nonsignificant decreases in frequency of parent-reported seizures in children with LGS.[35] A case series study showed 50% seizure reduction reported in almost half of children with LGS after 1 year of ketogenic diet. However, the strength of the study is challenged because it represents reports rather than scientific analysis of the clinical outcomes such as in a randomized controlled trial.[36]
Prognosis
The mortality rate ranges 3–7% in a mean follow up period of 8.5 to 9.7 years. Death is often related to accidents.[37]
Epidemiology
LGS is seen in approximately 4% of children with epilepsy, and is more common in males than in females.[13] Usual onset is between the ages of three and five.[7] Children can have no neurological problems prior diagnosis, or have other forms of epilepsy. West syndrome is diagnosed in 20% of patients before it evolves into LGS at about 2 years old.[14]
Finland
According to a 1997 community-based retrospective study in the Helsinki metropolitan area and the province of Uusimaa, the annual incidence of Lennox–Gastaut was 2 in 100,000 (0.002%) from 1975 to 1985.[38]
United States
0.026% of all children in the Atlanta, Georgia metropolitan area were estimated to have LGS in 1997, which was defined as, "onset of multiple seizure types before age 11 years, with at least one seizure type resulting in falls, and an EEG demonstrating slow spike-wave complexes (<2.5 Hz)." The study concluded that LGS accounts for 4% of childhood epilepsies.[13]
Research
Vigabatrin was found by Feucht et al. to be an effective add-on in patients whose seizures were not satisfactorily controlled by valproate. Out of 20 children, only 1 experienced a serious side effect (dyskinesia).[39]
Zonisamide showed promise in an overview of controlled and uncontrolled trials conducted in Japan.[40] However, in a physician survey conducted December 2004, only 28% of Lennox–Gastaut and West syndrome patients improved on zonisamide.[41]
Soticlestat is an investigational anticonvulsant that was well tolerated and reduced seizure frequency in a phase 2 clinical study for the treatment of Lennox-Gastaut syndrome[42][43][44] and began phase 3 trials in 2022.[44]
Lennox-Gastaut Syndrome Foundation
The Lennox-Gastaut Syndrome (LGS) Foundation, based in San Diego, California, is dedicated to improving the lives of those impacted by LGS through advancing research, awareness, education, and family support. The organization's slogan is: "The challenges are tough. So are we".[45]
References
- 1 2 3 Specchio, Nicola; Wirrell, Elaine C.; Scheffer, Ingrid E.; Nabbout, Rima; Riney, Kate; Samia, Pauline; Guerreiro, Marilisa; Gwer, Sam; Zuberi, Sameer M.; Wilmshurst, Jo M.; Yozawitz, Elissa; Pressler, Ronit; Hirsch, Edouard; Wiebe, Samuel; Cross, Helen J. (June 2022). "International League Against Epilepsy classification and definition of epilepsy syndromes with onset in childhood: Position paper by the ILAE Task Force on Nosology and Definitions". Epilepsia. 63 (6): 1398–1442. doi:10.1111/epi.17241. ISSN 0013-9580. PMID 35503717. S2CID 248503776.
- ↑ Markand, Omkar N. (2003-12-01). "Lennox–Gastaut syndrome (childhood epileptic encephalopathy)". Journal of Clinical Neurophysiology. 20 (6): 426–441. doi:10.1097/00004691-200311000-00005. ISSN 0736-0258. PMID 14734932. S2CID 46515787.
- ↑ Archer, John S.; Warren, Aaron E. L.; Jackson, Graeme D.; Abbott, David F. (2014-01-01). "Conceptualizing Lennox–Gastaut syndrome as a secondary network epilepsy". Frontiers in Neurology. 5: 225. doi:10.3389/fneur.2014.00225. PMC 4214194. PMID 25400619.
- ↑ Asadi-Pooya, Ali A. (March 2018). "Lennox-Gastaut syndrome: a comprehensive review". Neurological Sciences. 39 (3): 403–414. doi:10.1007/s10072-017-3188-y. ISSN 1590-3478. PMID 29124439. S2CID 4243468.
- ↑ Dravet, C., & Roger, J. (1996). Henri Gastaut 1915-1995. Epilepsia, 37(4), 410–415. https://doi.org/10.1111/j.1528-1157.1996.tb00580.x
- ↑ "LGS Foundation | Lennox-Gastaut Syndrome".
- 1 2 Bourgeois, Blaise F. D.; Douglass, Laurie M.; Sankar, Raman (2014-09-01). "Lennox–Gastaut syndrome: a consensus approach to differential diagnosis" (PDF). Epilepsia. 55 (Suppl 4): 4–9. doi:10.1111/epi.12567. ISSN 1528-1167. PMID 25284032. S2CID 27913979.
- ↑ Albert P. Aldenkamp, Fritz E. Dreifuss, W. Renier, T.P.B.M. Suurmeijer, Epilepsy in Children and Adolescents. Pg. 51
- ↑ Ohtahara S, Yamatogi Y, Ohtsukd Y, Oka E, lshida T. Prognosis of West syndrome with special reference to Lennox syndrome: a developmental study. In: Wada JA, Penry JK, eds. Advunces in epileptology: The Xth Epilepsy International Symposium. New York: Raven Press, 1980: 149–54
- ↑ "Epilepsy: Type of Seizures and Their Symptoms". MedicineNet.
- ↑ "Lennox-Gastaut Syndrome - an overview | ScienceDirect Topics". www.sciencedirect.com. Retrieved 2022-02-11.
- ↑ Panayiotopoulos, C. P. (2005). Neonatal Seizures and Neonatal Syndromes. Bladon Medical Publishing.
- 1 2 3 Trevathan, E; Murphy, CC; Yeargin-Allsopp, M (1997). "Prevalence and descriptive epidemiology of Lennox–Gastaut syndrome among Atlanta children". Epilepsia. 38 (12): 1283–8. doi:10.1111/j.1528-1157.1997.tb00065.x. PMID 9578523. S2CID 10245400.
- 1 2 3 4 Tyagi, Satyanand; et al. (Jul–Sep 2010). "Pharmacological Management of Lennox–Gastaut Syndrome a Difficult to Treat Form of Childhood-Onset Epilepsy: An Overview" (PDF). International Journal of Pharma and Bio Sciences. 1 (3): 1–6. Archived from the original (PDF) on 2018-07-08. Retrieved 2013-09-12.
- ↑ Lund C, Brodtkorb E, Øye AM, Røsby O, Selmer KK (2014). "CHD2 mutations in Lennox–Gastaut syndrome". Epilepsy Behav. 33: 18–21. doi:10.1016/j.yebeh.2014.02.005. PMID 24614520. S2CID 140207920.
- ↑ LCapelli LP, Krepischi AC, Gurgel-Giannetti J, Mendes MF, Rodrigues T, Varela MC, Koiffmann CP, Rosenberg C (2012). "Deletion of the RMGA and CHD2 genes in a child with epilepsy and mental deficiency". Eur J Med Genet. 55 (2): 132–134. doi:10.1016/j.ejmg.2011.10.004. PMID 22178256.
- ↑ Allen AS, Berkovic SF, Cossette P, et al. (2013-09-12). "De novo mutations in the classic epileptic encephalopathies". Nature. 501 (7466): 217–221. doi:10.1038/nature12439. ISSN 0028-0836. PMC 3773011. PMID 23934111.
- ↑ Lund, Caroline; Brodtkorb, Eylert; Røsby, Oddveig; Rødningen, Olaug Kristin; Selmer, Kaja Kristine (2013-07-01). "Copy number variants in adult patients with Lennox–Gastaut syndrome features". Epilepsy Research. 105 (1–2): 110–117. doi:10.1016/j.eplepsyres.2013.01.009. ISSN 1872-6844. PMID 23415449. S2CID 6221643.
- ↑ Choi MH, Yang JO, Min JS, Lee JJ, Jun SY1, Lee YJ, Yoon JY, Jeon SJ, Byeon I, Kang JW, Kim NS (2019) A novel X-linked variant of IQSEC2 is associated with Lennox-Gastaut syndrome and mild intellectual disability in three generations of a Korean Family. Genet Test Mol Biomarkers
- ↑ Brigo F, Jones K, Eltze C, Matricardi S (7 April 2021). "Anti-seizure medications for Lennox-Gastaut syndrome". The Cochrane Database of Systematic Reviews. 2021 (4): CD003277. doi:10.1002/14651858.CD003277.pub4. PMC 8095011. PMID 33825230.
- ↑ Motte, J; Trevathan, E; Arvidsson, JF; Barrera, MN; Mullens, EL; Manasco, P (1997). "Lamotrigine for generalized seizures associated with the Lennox–Gastaut syndrome. Lamictal Lennox–Gastaut Study Group". The New England Journal of Medicine. 337 (25): 1807–12. doi:10.1056/NEJM199712183372504. PMID 9400037.
- ↑ Epilepsy Ontario (1999). "Lamotrigine Approved in Canada for Lennox–Gastaut Syndrome". 'Sharing' News. Archived from the original on 4 February 2012. Retrieved 13 November 2005.
- ↑ Glaxo Wellcome Inc (1998). "Final Printed Labeling—Part 1". Lamictal Tablets & Chewable Dispersible Tablets (Lamotrigine) Drug Approval Page. United States Food and Drug Administration Center for Drug Evaluation and Research. Archived from the original on April 29, 2005. Retrieved 13 November 2005.
- ↑ Sachdeo, R. C.; Glauser, TA; Ritter, F; Reife, R; Lim, P; Pledger, G (1999). "A double-blind, randomized trial of topiramate in Lennox–Gastaut syndrome". Neurology. 52 (9): 1882–7. doi:10.1212/wnl.52.9.1882. PMID 10371538. S2CID 73000217.
- ↑ Alva-Moncayo, E; Ruiz-Ruiz, A (2003). "Utilidad del topiramato como terapia añadida a esquemas convencionales para el síndrome de Lennox–Gastaut" [The value of topiramate used with conventional schemes as an adjunctive therapy in the treatment of Lennox–Gastaut syndrome]. Revista de Neurología (in Spanish). 36 (5): 453–7. doi:10.33588/rn.3605.2002014. PMID 12640599.
- ↑ "Felbatol (felbamate)". p. 3. Archived from the original on 2007-11-09. Retrieved 2007-09-19.
- ↑ The Felbamate Study Group In Lennox–Gastaut Syndrome (1993). "Efficacy of felbamate in childhood epileptic encephalopathy (Lennox-Gastaut syndrome). The Felbamate Study Group in Lennox–Gastaut Syndrome". The New England Journal of Medicine. 328 (1): 29–33. doi:10.1056/NEJM199301073280105. PMID 8347179.
- ↑ Devinsky, O; Faught, RE; Wilder, BJ; Kanner, AM; Kamin, M; Kramer, LD; Rosenberg, A (1995). "Efficacy of felbamate monotherapy in patients undergoing presurgical evaluation of partial seizures". Epilepsy Research. 20 (3): 241–6. doi:10.1016/0920-1211(94)00084-A. PMID 7796796. S2CID 21915205.
- ↑ O'neil, MG; Perdun, CS; Wilson, MB; Mcgown, ST; Patel, S (1996). "Felbamate-associated fatal acute hepatic necrosis". Neurology. 46 (5): 1457–9. doi:10.1212/wnl.46.5.1457. PMID 8628501. S2CID 46504929.
- 1 2 3 4 5 Cross, J. Helen; Auvin, Stéphane; Falip, Mercè; Striano, Pasquale; Arzimanoglou, Alexis (2017). "Expert Opinion on the Management of Lennox-Gastaut Syndrome: Treatment Algorithms and Practical Considerations". Frontiers in Neurology. 8: 505. doi:10.3389/fneur.2017.00505. ISSN 1664-2295. PMC 5649136. PMID 29085326.
- ↑ Auvin, Stéphane; Nortvedt, Charlotte; Fuller, Douglas S.; Sahebkar, Farhad (2023-04-13). "Seizure-free days as a novel outcome in patients with Lennox-Gastaut syndrome: Post hoc analysis of patients receiving cannabidiol in two randomized controlled trials". Epilepsia. 64 (7): 1812–1820. doi:10.1111/epi.17618. ISSN 1528-1167. PMID 37052803. S2CID 258111465.
- ↑ Douglass, LM (2014). "Surgical options for patients with Lennox–Gastaut syndrome". Epilepsia. 55: 21–28. doi:10.1111/epi.12742. PMID 25284034.
- ↑ Lee, Yun Jin (2010). "Resective pediatric epilepsy surgery in Lennox–Gastaut syndrome". Pediatrics. 125 (1): e58–e66. doi:10.1542/peds.2009-0566. PMID 20008422. S2CID 4836738.
- ↑ Liu, SY (2012). "Surgical treatment of patients with Lennox–Gastaut syndrome phenotype". The Scientific World Journal. 2012: 614263. doi:10.1100/2012/614263. PMC 3353538. PMID 22629163.
- ↑ Freeman, John M. (February 2009). "Seizures, EEG events, and the ketogenic diet". Epilepsia. 50 (2): 329–330. doi:10.1111/j.1528-1167.2008.01757.x. ISSN 1528-1167. PMID 19215282. S2CID 42564247.
- ↑ Cross, J. Helen (May 2012). "The ketogenic diet in the treatment of Lennox-Gastaut syndrome". Developmental Medicine and Child Neurology. 54 (5): 394–395. doi:10.1111/j.1469-8749.2012.04276.x. ISSN 1469-8749. PMID 22443688. S2CID 21003078.
- ↑ Glauser, Tracy A.; Morita, Diego A. (2002). "Introduction". Lennox–Gastaut Syndrome. eMedicine.com, Inc. Retrieved 8 July 2005.
- ↑ Heiskala, H (1997). "Community-based study of Lennox–Gastaut syndrome". Epilepsia. 38 (5): 526–31. doi:10.1111/j.1528-1157.1997.tb01136.x. PMID 9184597. S2CID 23615713.
- ↑ Feucht, M; Brantner-Inthaler, S (1994). "Gamma-vinyl-GABA (vigabatrin) in the therapy of Lennox–Gastaut syndrome: an open study". Epilepsia. 35 (5): 993–8. doi:10.1111/j.1528-1157.1994.tb02544.x. PMID 7925171. S2CID 24204172.
- ↑ Yagi, K (2004). "Overview of Japanese experience-controlled and uncontrolled trials". Seizure: The Journal of the British Epilepsy Association. 13 (Suppl 1): S11–5, discussion S16. doi:10.1016/j.seizure.2004.04.018. PMID 15511680.
- ↑ Yamauchi, T; Aikawa, H (2004). "Efficacy of zonisamide: our experience". Seizure: The Journal of the British Epilepsy Association. 13 (Suppl 1): S41–8, discussion S49. doi:10.1016/j.seizure.2004.04.021. PMID 15511689.
- ↑ Hahn CD, Jiang Y, Villanueva V, Zolnowska M, Arkilo D, Hsiao S, Asgharnejad M, Dlugos D (October 2022). "A phase 2, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of soticlestat as adjunctive therapy in pediatric patients with Dravet syndrome or Lennox-Gastaut syndrome (ELEKTRA)". Epilepsia. 63 (10): 2671–2683. doi:10.1111/epi.17367. PMC 9804149. PMID 35841234.
- ↑ Hong W, Haviland I, Pestana-Knight E, Weisenberg JL, Demarest S, Marsh ED, Olson HE (June 2022). "CDKL5 Deficiency Disorder-Related Epilepsy: A Review of Current and Emerging Treatment". CNS Drugs. 36 (6): 591–604. doi:10.1007/s40263-022-00921-5. PMC 9876658. PMID 35633486.
- 1 2 Pong AW, Ross J, Tyrlikova I, Giermek AJ, Kohli MP, Khan YA, Salgado RD, Klein P (March 2022). "Epilepsy: expert opinion on emerging drugs in phase 2/3 clinical trials". Expert Opinion on Emerging Drugs. 27 (1): 75–90. doi:10.1080/14728214.2022.2059464. PMID 35341431.
- ↑ Lennox-Gastaut Syndrome Foundation, accessed 5 December 2023