| Long COVID | |
|---|---|
| Other names | Long-haul COVID, post-COVID-19 syndrome, post-COVID-19 condition, post-acute sequelae of COVID-19 (PASC), chronic COVID syndrome[1] |
| Symptoms | Highly varied, including post-exertional malaise (symptoms worsen with effort), fatigue, muscle pain, shortness of breath, chest pain and cognitive dysfunction ("brain fog")[2] |
| Duration | Weeks to years, possibly lifelong[3] |
| Causes | COVID-19 infection |
| Risk factors | Female sex, age, obesity, asthma, more severe COVID-19 infection[4] |
| Frequency | 50–70% of hospitalised COVID-19 cases, 10–30% of non-hospitalised cases, and 10–12% of vaccinated cases[3] |
Long COVID or long-haul COVID is a group of health problems persisting or developing after an initial COVID-19 infection. Symptoms can last weeks, months or years and are often debilitating.[3] The World Health Organization defines long COVID as starting three months after infection, but other definitions put the start of long COVID at four weeks.[2]
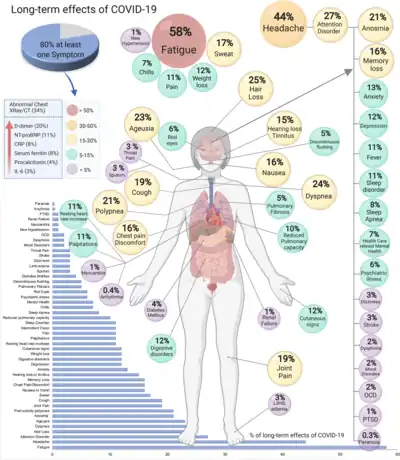
Long COVID is characterised by a large number of symptoms, which sometimes disappear and reappear. Commonly reported symptoms of long COVID are fatigue, memory problems, shortness of breath, and sleep disorder.[5][6][7] Many other symptoms can also be present, including headaches, loss of smell or taste, muscle weakness, fever, and cognitive dysfunction and problems with mental health.[5][7] Symptoms often get worse after mental or physical effort, a process called post-exertional malaise.[5] There is a large overlap in symptoms with ME/CFS.[2]
The causes of long COVID are not yet fully understood. Hypotheses include lasting damage to organs and blood vessels, problems with blood clotting, neurological dysfunction, persistent virus or a reactivation of latent viruses and autoimmunity.[3] Diagnosis of long COVID is based on suspected or confirmed COVID-19 infection, symptoms and by excluding alternative diagnoses.[8][9]
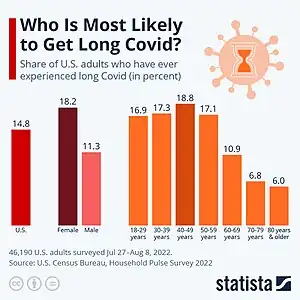
Estimates of the prevalence of long COVID vary based on definition, population studied, time period studied, and methodology, generally ranging between 5% and 50%.[10] Prevalence is less after vaccination.[11] Risk factors are higher age, female sex, having asthma, and a more severe initial COVID-19 infection.[4] As of 2023, there are no established disease-modifying treatments.[3][5] Management of long COVID depends on symptoms. Rest is recommended for fatigue and pacing for post-exertional malaise. People with severe symptoms or those who were in intensive care may require care from a team of specialists.[12] Most people with symptoms at 4 weeks recover by 12 weeks. Recovery for those still ill at 12 weeks is slower or plateaus.[12] For a subset of people, for instance those meeting the criteria for ME/CFS, symptoms are expected to be lifelong.[3]
Classification and terminology
Long COVID is a patient-created term coined early in the pandemic by those suffering from long-term symptoms.[13][14] While long COVID is the most prevalent name, the terms long-haul COVID, post-COVID-19 syndrome, post-COVID-19 condition,[1][15] post-acute sequelae of COVID-19 (PASC), and chronic COVID syndrome are also in use.[5]
Long COVID may not be a single disease or syndrome. It could be an umbrella term including permanent organ damage, post-intensive care syndrome, post-viral fatigue syndrome and post-COVID syndrome.[2]
Clinical case definitions
There are multiple definitions of long COVID, depending on country and institution. The most accepted is the World Health Organization (WHO) definition.[16]
The definitions differ in when long COVID starts, and how long persistent symptoms must have lasted.[16] For instance, the WHO puts the onset of long COVID at three months post-infection, if there have been at least 2 months of persistent symptoms.[1][15] In contrast, the US Centers for Disease Control and Prevention (CDC) puts the onset of "Post-COVID Conditions" at 4 weeks "to emphasize the importance of initial clinical evaluation and supportive care during the initial 4 to 12 weeks after acute COVID-19"[8]
The British National Institute for Health and Care Excellence (NICE) divides long COVID into two categories:[17]
- ongoing symptomatic COVID-19 for effects from four to twelve weeks after onset, and
- post-COVID-19 syndrome for effects that persist 12 or more weeks after onset.
The case definitions specify symptom onset and development. For instance, the WHO definition indicates that "symptoms might be new onset following initial recovery or persist from the initial illness. Symptoms may also fluctuate or relapse over time."[1]
The NICE and WHO definition further require the exclusion of alternative diagnoses.[16]
Related illnesses

Long COVID is a post-acute infection syndrome (PAIS) and shares similarities with other such syndromes.[18] For instance, there are similarities with post-Ebola syndrome and aftereffects of the chikungunya virus. These conditions may have similar pathophysiology to long COVID.[18][19] Post-COVID-19 research has also found influenza can have longer-lived negative effects, though to a much smaller degree than COVID-19, leading to the moniker "long flu".[20]
Long COVID has many symptoms in common with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and research estimates half of people with long COVID meet ME/CFS diagnostic criteria.[21] Like long COVID, ME/CFS is often triggered by infections, and some biological changes overlap.[22][2] Dysautonomia and postural orthostatic tachycardia syndrome (POTS) are also potential shared aspects of long COVID and ME/CFS.[2]
Signs and symptoms
| External videos | |
|---|---|
There is a large set of symptoms associated with long COVID, impacting many different organs and body systems. Long COVID symptoms can differ significantly from person to person.[2] Symptom severity ranges from mild to incapacitating.[24]
Common symptoms reported in studies include fatigue, muscle pain, shortness of breath, chest pain, cognitive dysfunction ("brain fog") and post-exertional malaise (symptoms worsen after activity).[2] This symptom worsening typically occurs 12 to 48 hours after activity and can be triggered by either mental or physical effort. It lasts between days and weeks.[8]
Neurological symptoms
Common neurological symptoms in long COVID are difficulty concentrating, cognitive impairment and headaches.[3][7] People also frequently experience loss of taste and loss of smell.[7]
Some people with long COVID experience dysautonomia, a malfunction of the central nervous system.[25] People with dysautonomia may experience palpitations and tachycardia (raised heart rate) after minor effort or upon standing up. This can be associated with dizziness and nausea. If the heart rate is raised by 30 beats per minute or more after standing in a sustained way, this is described as postural orthostatic tachycardia syndrome.[26]
In terms of mental health, people with long COVID often experience sleep difficulties.[7] A large study showed that depression and anxiety levels are raised in the first two months after infection, but return to normal afterwards. This was in contrast to other neurological symptoms, such as brain fog and seizures, which lasted at least two years.[3]
Lungs, heart and digestive system
A 2022 review found difficulty breathing as the second-most common symptom of long COVID.[27] People can also experience a persistent cough.[7] Less frequently, people with long COVID experience diarrhea and nausea.[7]
In the cardiovascular system, effort intolerance and chest pain occur often in people with long COVID.[7] People are at increased risk of stroke, pulmonary embolism and myocardial infarction after recovering from an acute COVID infection, but there is disagreement as to whether this should be seen as part of long COVID or not.[2]
Other symptoms
Joint pain and muscle pain are frequently reported as symptoms of long COVID.[7] Some people experience hair loss and skin rashes.[28] People are at increased risk of type I and II diabetes after recovering from acute COVID.[2]
Subgroups
Because the symptom combinations of long COVID vary significantly from person to person, one approach to researching the condition is to define subgroups or clusters of long-haulers. This would allow for more targeted clinical care.[2]
Causes and mechanisms
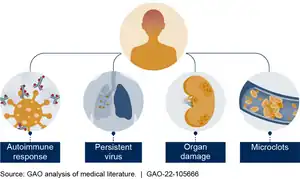
The causes of long COVID are not yet fully understood. It is likely that there is no single cause, but instead multiple, and possibly overlapping, mechanisms that all contribute to the development of long COVID.[3] Organ damage from the acute infection can explain a part of the symptoms, but long COVID is also observed in people where organ damage seems to be absent.[29] Several hypotheses have been put forward explaining long COVID. A 2023 review article included:[3]
- blood clotting and endothelial dysfunction in the blood vessels
- neurological issues: problems with signalling from the brainstem and the vagus nerve
- immune system dysregulation, including the reactivation of viruses like the Epstein–Barr virus
- impacts of the virus on the microbiota, including viral persistence
- autoimmunity
Further hypotheses include a dysfunction of the mitochondria and the cellular energy system,[30] persistent systemic inflammation, and the persistence of SARS-COV-19 antigens.[31]
Pathophysiology
Organ damage from the acute infection may explain symptoms in some people with long COVID. Radiological tests such as lung MRIs often show up as normal even for people who show clear desaturation (lowered blood oxygen level) after mild exercise. Other tests, such as a dual-energy CT scan, do show perfusion defects in a subset of people with respiratory symptoms. Imaging of the heart show contradictory results. Imaging of brains show changes after COVID infection, even if this has not been studied in relation to long COVID. For instance, some show a smaller olfactory bulb, a brain region associated with smell.[2]
In a subset of people with long COVID, there is evidence that SARS-COV-2 remains in the body after the acute infection.[32] This evidence comes from biopsies, studies of blood plasma, and by the indirect immune effects of persistent virus. Viral DNA or proteins have been found months to a year after acute infection in various studies. A small study demonstrated viral RNA up to nearly two years after an acute infection in people with long COVID. Persistent virus has also been found in people without long COVID, even though at a lower rate.[33] Persistent virus could lead to symptoms via possible effects on coagulation and via microbiome and neuroimmune abnormalities.[34]
During or after acute COVID infection, various dormant viruses can become reactivated. For instance, SARS-COV-2 can reactivate the Epstein-Barr virus, the virus that is responsible for mono. This virus lies dormant in most people. There is some evidence of a relationship between its reactivation and long COVID. A correlation was also found between reactivation of endogenous retroviruses and severity of active COVID-19.[35]
Autoimmunity is another potential cause of long COVID. Some studies report auto-antibodies (antibodies directed against an individual's own proteins) in people with long COVID, but they are not found in all studies.[31] Autoantibodies are often induced during acute COVID, with a moderate relationship to disease severity. Evidence from electronic health care records show that people develop auto-immune diseases, such as lupus and rheumatoid arthritis, more frequently after a COVID-19 infection, compared to controls.[2]
Issues with increased blood clotting are another potential driver of long COVID development. During acute infection, there is direct damage to the linings of blood vessels (endothelial damage),[2] and the risk of thrombosis-related diseases stays elevated longer-term after infection. Issues with blood clotting can include hyperactive platelets and microclots. These microclots may induce oxygen shortage (hypoxia) in tissues.[32] The clotting may potentially be driven by autoantibodies.[2]
Risk factors
Women are more at risk then men.[4] Age has been identified as another risk factor, with older people seemingly more at risk.[4] This is also true for children, with older children at a higher risk than younger children.[16] Most diagnoses of long COVID are in the 36–50 age bracket.[3] Risks of developing long COVID are also higher for people with lower incomes, people with fewer years of education and those from disadvantaged ethnic groups.[16][32] People who smoke also have a higher risk of developing long COVID.[16]
Various health issues raise the risk of long COVID. For instance, people with obesity more often report long COVID.[4] Asthma and chronic obstructive pulmonary disease are also risk factors.[16][4] In terms of mental health, depression and anxiety raise risks.[16]
Finally, characteristics of the acute infection play a role in developing long COVID. People who experience a larger number of symptoms during the acute infection are more likely to develop long COVID, as well as people who require hospitalisation.[4] Finally, long COVID risks may have been higher with the SARS-CoV2 Delta variant compared to the Omicron variant. The higher infection rate from the Omicron variant means that it is still responsible for a large group of long-haulers.[16]
Diagnosis
There are no standardised tests to determine if symptoms persisting after COVID-19 infection are due to long COVID.[5][9] Diagnosis is based on a history of suspected or confirmed COVID-19 symptoms, and by considering and ruling out alternative diagnoses.[8][9] Diagnosis of long COVID can be challenging because of the wide range of symptoms people with long COVID may display.[9]
Early diagnostic criteria of long COVID required a laboratory-confirmed COVID-19 infection, but current criteria do not require this anymore, given that people may not get tested during the acute infection.[9] For instance, people who develop long COVID after asymptomatic infection would have little reason to get tested.[8] Furthermore, tests for COVID are not foolproof, and can come back negative.[8] False negatives are more common for children, women and people with a low viral load.[3]
There are diagnostic tools available for some elements of long COVID, such as the tilt table test for POTS and MRI scans to test for cardiovascular impairment. Routine tests offered in standard care often come back normal.[3]
Prevention
Preventing a COVID-19 infection is the most effective way to prevent long COVID, for instance by improving ventilation, avoiding contact with people who test positive for COVID, washing hands, and wearing a properly-fitted N95 mask.[36] Treatment during the acute phase may also reduce the risk of long COVID.[5]
COVID-19 vaccination reduces the risk of long COVID, but by how much is unclear, as the available studies differ widely and are of limited quality.[11] One complication is that healthy people more often opt to get vaccinated, which makes it more difficult to draw conclusions on the effect of vaccination.[37] A 2023 review found that three doses of a COVID-19 vaccine offer 69% effectiveness against long COVID, while two doses had 37% efficacy, for those who had not been infected with COVID-19 before.[38][39]
Clinical care
As of 2023 there are no established effective treatments for long COVID,[3] however several countries and medical organizations have produced guidelines on long COVID for clinicians and the public.[5][40][41]
People with long COVID may need care within several clinical disciplines for long-term monitoring or intervention of ongoing symptoms, and to implement social services, physical therapy, or mental health care.[41] In some countries, such as the UK and Germany, specialised long COVID outpatient clinics have been established to assess individual cases for the extent of surveillance and treatment needed.[42] Two reviews indicated that primary physicians should provide the first assessment of people with long COVID symptoms, leading to specialist referrals for more complex long COVID symptoms.[41][42]
Management of long COVID depends on symptoms.[5] Rest, planning and prioritising are advised for people with fatigue. People who get post-exertional malaise may benefit from activity management with pacing. People with allergic-type symptoms, such as skin rashes, may benefit from antihistamines.[12] Those with autonomic dysfunction may benefit from increased intake of fluids, electrolytes and compression garments.[12]
Long-term follow-up of people with long COVID involves outcome reports from the people themselves to assess the impact on their quality of life, especially for those who were not hospitalised and receiving regular clinical follow-up.[41][42] Digital technologies, such as videoconferencing, are being implemented between primary care physicians and people with long COVID as part of long-term monitoring.[41]
Prognosis
Around two in three with symptoms at four weeks are expected to recover fully by week twelve.[12] However, the prognosis varies by person, and some may find symptoms worsen within the first three months.[8] Recovery after twelve weeks is variable: some people plateau, whilst others see a slow recovery.[12]
The prognosis also varies by symptom: neurological symptoms may have a delayed onset, and some get worse over time. Symptoms of the gut and lungs are more likely to reduce over time. Pain in muscles and joints seems worse at 2 years than at 1 year after infection. If people meet the diagnostic criteria for ME/CFS or for dysautonomia, it is possible that symptoms are lifelong.[3]
Epidemiology
Estimates of the prevalence of long COVID vary widely. The estimates depend on the definition of long COVID and the population studied.[4] A conservative estimate based only on confirmed COVID cases puts the global number of people with long COVID at 65 million.[3] While hospitalised people have higher risks of getting long COVID, most long-haulers had a mild infection and were able to recover from the acute infection at home.[3]
An April 2022 meta-analysis estimated that the pooled prevalence of post-COVID conditions after infection was 43%, with estimates ranging between 9% and 81%. People who had been hospitalised with COVID saw a higher prevalence of 54%, while 34% of nonhospitalised people developed long COVID after acute infection.[4]
In the United States in June 2023, 6% of the population indicated having long COVID, as defined as symptoms that last for 3 months or more.[43] This percentage had stayed stable since January that year, but was a decrease compared to June 2022.[43] Of people who had had a prior COVID infection, 11% indicated having long COVID. A quarter of those reported significant limitation in activity.[43]
In a large population cohort study in Scotland, 42% of respondents said they had not fully recovered after 6 to 18 months after catching COVID, and 6% indicated they had not recovered at all. The risk of long COVID was associated with disease severity; people with asymptomatic infection did not have increased risk of long COVID symptoms compared to people who had never been infected. Those that had been hospitalised had 4.6 times higher odds of no recovery compared to nonhospitalised people.[44]
Children and adolescents
Long COVID is less common in children and adolescents than in adults.[45] A 2023 systemic review estimated the differences in persistent symptom frequency between children and adolescents who tested positive for COVID, and controls. The pooled proportion of children and adolescents experiencing three or more persistent symptoms after a COVID infection was 17% more than the controls. The largest differences were found for loss of smell or distorted smell, anxiety and fatigue.[46] Another 2023 review found a prevalence of 16.2% in children and adolescents at least 3 months after infection. The most common symptoms found in this review were a persistent fever, sore throat, problems with sleep, muscle weakness and fatigue.[47] Although Long COVID is less common in children and adolescents, a 2023 study found that children and adolescents can experience serious symptoms and long-term adverse health effects, including serious mental health impacts related to persistent COVID-19 symptoms.[48]
Society and culture
Patient community and activism
Early in the pandemic, official guidance made a distinction between those with mild illness who did not require hospitalisation, and those with severe illness which did require hospitalisation. The typical recovery time for those with mild illness was said to be around two weeks[49] and media attention was mostly focused on those with a severe infection. Patients with long-lasting systems after a mild infection started to describe their symptoms on Twitter and blogs,[50] challenging official assumptions.[51]
The term long COVID was reportedly first used in May 2020 as a hashtag on Twitter by Elisa Perego, a health and disability researcher at University College London.[13][51] A month later, #LongCovid became a popular hashtag, alongside hashtags from non-English budding communities (for instance, #AprèsJ20 in French, and #koronaoire in Finnish).[51]
Experiences shared online filled a gap in knowledge in how the media talked about the pandemic.[50] Via the media, the knowledge reached governments and health officials, making long COVID "the first illness created through patients finding one another on Twitter".[51]
Some people experiencing long COVID have formed community care networks and support groups on social media websites.[42][52] Internationally, there are several long COVID advocacy groups.[41][53][54][55] Clinical advice on self-management and online healthcare programs are used to support people with long COVID.[42]
Stigma and discrimination
Many people with long COVID have difficulty accessing appropriate healthcare. The severity of their symptoms may be disbelieved, they may be subject to unsympathetic care, and their symptoms may not be investigated properly or may be falsely attributed to anxiety.[56][41] People with long COVID may be misdiagnosed with mental disorders. Anxiety and depression questionnaires not designed for people with medical conditions can contribute to this; for example, a questionnaire may assume fatigue is due to depression or that palpitations are due to anxiety, even if explained by another condition like ME/CFS or POTS.[3]
Work-related impacts
The impact of long COVID on people's ability to work is large. Estimates vary on how many people are out of work, or work reduced hours because of long COVID. For those with mild or moderate disease, between 12% and 23% had had long periods of absence or remained absent from work at 3 to 7 months. The share of people working adjusted hours or tasks after mild or moderate COVID, was around 8% to 45% after three to eight months.[57] The percentage of people returning to work after hospitalisation was lower.[57] Return to work after hospitalisation differed by country. In China and the US a higher percentage went back to work. In the US this could be partially explained by a lack of paid sick leave for some workers.[58] The Institute for Fiscal Studies studied labour impacts of long COVID in the UK in 2021. They concluded that of people who worked before contracting long COVID, one in ten had stopped working. Most of them were on sick leave rather than unemployed.[59]
Research
As long COVID is a novel condition, open questions abound. Research is ongoing in many areas, including developing more accurate diagnostic criteria, refining estimates of its likelihood, identifying risk factors, gathering data for its impact on daily life, discovering which populations face barriers to adequate care, and learning how much protection vaccination provides.[60][61]
Many experimental and repurposed drugs are being investigated as possible treatments for different aspects of long COVID.[3][62] These include the anti-inflammatory colchicine, the anticoagulant rivaroxaban, the antihistamines famotidine and loratadine, various immune-modulating drugs, and the experimental aptamer compound BC-007.[2][3]
In 2021, the US National Institutes of Health started funding the RECOVER Initiative, backed by $1.15 billion over four years,[63] to identify the causes, prevention and treatment of long COVID.[24] In 2023, the Office of Long COVID Research and Practice was created to coordinate research across US government agencies.[64] At the same time, RECOVER announced which clinical trials it will fund: these include a trial of Paxlovid against potential persistent infection, one for sleep disorder, one for cognitive impairment and one for problems with the autonomic nervous system.[65]
In a 2023 survey of 3,700 people with long COVID, fatigue was the symptom most closely associated with poor everyday functioning, while quality of life, depression and brain fog also occurred.[66] Some 20% of people with long COVID were unable to work.[66][67]
See also
- Impact of the COVID-19 pandemic on neurological, psychological and other mental health outcomes – both acute and chronic neurological, psychiatric, olfactory, and mental health conditions
- List of people with long COVID
- Multisystem inflammatory syndrome in children – pediatric comorbidity from COVID-19
- Post viral cerebellar ataxia – clumsy movement appearing a few weeks after a viral infection
References
- 1 2 3 4 Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV (April 2022). "A clinical case definition of post-COVID-19 condition by a Delphi consensus". The Lancet. Infectious Diseases. 22 (4): e102–e107. doi:10.1016/S1473-3099(21)00703-9. PMC 8691845. PMID 34951953.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Altmann DM, Whettlock EM, Liu S, Arachchillage DJ, Boyton RJ (July 2023). "The immunology of long COVID". Nature Reviews. Immunology. 23 (10): 618–634. doi:10.1038/s41577-023-00904-7. PMID 37433988. S2CID 259831825.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Davis HE, McCorkell L, Vogel JM, Topol EJ (March 2023). "Long COVID: major findings, mechanisms and recommendations". Nature Reviews. Microbiology. 21 (3): 133–146. doi:10.1038/s41579-022-00846-2. PMC 9839201. PMID 36639608.
- 1 2 3 4 5 6 7 8 9 Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B (November 2022). "Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review". The Journal of Infectious Diseases. 226 (9): 1593–1607. doi:10.1093/infdis/jiac136. PMC 9047189. PMID 35429399.
- 1 2 3 4 5 6 7 8 9 "Long COVID or post-COVID conditions". Centers for Disease Control and Prevention, US Department of Health and Human Services. 2023-07-20. Retrieved 2023-07-23.
- ↑ Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B (November 2022). "Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review". The Journal of Infectious Diseases. 226 (9): 1593–1607. doi:10.1093/infdis/jiac136. PMC 9047189. PMID 35429399.
- 1 2 3 4 5 6 7 8 9 Alkodaymi MS, Omrani OA, Fawzy NA, Shaar BA, Almamlouk R, Riaz M, et al. (May 2022). "Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: a systematic review and meta-analysis". Clinical Microbiology and Infection. 28 (5): 657–666. doi:10.1016/j.cmi.2022.01.014. PMC 8812092. PMID 35124265.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 3 4 5 6 7 "Post-COVID Conditions: Information for Healthcare Providers". Centers for Disease Control and Prevention. 2022-12-16. Retrieved 2023-08-10.
- 1 2 3 4 5 Srikanth S, Boulos JR, Dover T, Boccuto L, Dean D (September 2023). "Identification and diagnosis of long COVID-19: A scoping review". Progress in Biophysics and Molecular Biology. 182: 1–7. doi:10.1016/j.pbiomolbio.2023.04.008. PMC 10176974. PMID 37182545.
- ↑ Ledford H (June 2022). "How common is long COVID? Why studies give different answers". Nature. 606 (7916): 852–853. Bibcode:2022Natur.606..852L. doi:10.1038/d41586-022-01702-2. PMID 35725828. S2CID 249887289.
- 1 2 Byambasuren O, Stehlik P, Clark J, Alcorn K, Glasziou P (2023). "Effect of covid-19 vaccination on long covid: systematic review". BMJ Medicine. 2 (1): e000385. doi:10.1136/bmjmed-2022-000385. PMC 9978692. PMID 36936268.
- 1 2 3 4 5 6 Greenhalgh T, Sivan M, Delaney B, Evans R, Milne R (September 2022). "Long covid-an update for primary care". BMJ. 378: e072117. doi:10.1136/bmj-2022-072117. PMID 36137612. S2CID 252406968.
- 1 2 Perego E, Callard F, Stras L, Melville-Johannesson B, Pope R, Alwan N (2020-10-01). "Why we need to keep using the patient made term 'Long Covid'". The BMJ. Archived from the original on 2020-10-04. Retrieved 2020-10-18.
- ↑ Callard F, Perego E (January 2021). "How and why patients made Long Covid". Social Science & Medicine. 268: 113426. doi:10.1016/j.socscimed.2020.113426. PMC 7539940. PMID 33199035.
- 1 2 "A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021". World Health Organization. Archived from the original on 2022-04-23. Retrieved 2022-01-07.
- 1 2 3 4 5 6 7 8 9 Su S, Zhao Y, Zeng N, Liu X, Zheng Y, Sun J, et al. (July 2023). "Epidemiology, clinical presentation, pathophysiology, and management of long COVID: an update". Molecular Psychiatry. doi:10.1038/s41380-023-02171-3. PMID 37491461. S2CID 260163143.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ "COVID-19 rapid guideline: managing the long-term effects of COVID-19". National Institute for Health and Care Excellence. 2021-11-11. p. 5. Retrieved 2023-09-09.
- 1 2 Choutka J, Jansari V, Hornig M, Iwasaki A (May 2022). "Unexplained post-acute infection syndromes". Nature Medicine. 28 (5): 911–923. doi:10.1038/s41591-022-01810-6. PMID 35585196. S2CID 248889597.
- ↑ Brodin P (January 2021). "Immune determinants of COVID-19 disease presentation and severity". Nature Medicine. 27 (1): 28–33. doi:10.1038/s41591-020-01202-8. PMID 33442016.
- ↑ Jamie Ducharme (2023-12-14). "You've Heard of Long COVID. Long Flu Is a Health Risk, Too". Time.
- ↑ Grach SL, Seltzer J, Chon TY, Ganesh R (October 2023). "Diagnosis and Management of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome". Mayo Clinic Proceedings. 98 (10): 1544–1551. doi:10.1016/j.mayocp.2023.07.032. PMID 37793728. S2CID 263665180.
- ↑ Komaroff AL, Lipkin WI (2023-06-02). "ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature". Frontiers in Medicine. 10. doi:10.3389/fmed.2023.1187163. ISSN 2296-858X. PMC 10278546. PMID 37342500.
- ↑ Lopez-Leon S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, et al. (August 2021). "More than 50 long-term effects of COVID-19: a systematic review and meta-analysis". Scientific Reports. 11 (1): 16144. Bibcode:2021NatSR..1116144L. doi:10.1038/s41598-021-95565-8. PMC 8352980. PMID 34373540.
- 1 2 "NIH launches new initiative to study 'Long COVID'". National Institutes of Health (NIH). 2021-02-23. Archived from the original on 2021-05-13. Retrieved 2021-02-23.
- ↑ Stefanou MI, Palaiodimou L, Bakola E, Smyrnis N, Papadopoulou M, Paraskevas GP, et al. (2022). "Neurological manifestations of long-COVID syndrome: a narrative review". Therapeutic Advances in Chronic Disease. 13: 20406223221076890. doi:10.1177/20406223221076890. PMC 8859684. PMID 35198136.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Espinosa-Gonzalez AB, Master H, Gall N, Halpin S, Rogers N, Greenhalgh T (February 2023). "Orthostatic tachycardia after covid-19". BMJ (Clinical Research Ed.). 380: e073488. doi:10.1136/bmj-2022-073488. PMID 36828559. S2CID 257103171.
- ↑ Healey Q, Sheikh A, Daines L, Vasileiou E (May 2022). "Symptoms and signs of long COVID: A rapid review and meta-analysis". Journal of Global Health. 12: 05014. doi:10.7189/jogh.12.05014. PMC 9125197. PMID 35596571.
- ↑ "COVID-19 rapid guideline: managing the long-term effects of COVID-19". National Institute for Health and Care Excellence. 2021-11-11. p. 100. Retrieved 2023-09-09.
- ↑ Castanares-Zapatero D, Chalon P, Kohn L, Dauvrin M, Detollenaere J, Maertens de Noordhout C, et al. (December 2022). "Pathophysiology and mechanism of long COVID: a comprehensive review". Annals of Medicine. 54 (1): 1473–1487. doi:10.1080/07853890.2022.2076901. PMC 9132392. PMID 35594336.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Astin R, Banerjee A, Baker MR, Dani M, Ford E, Hull JH, et al. (January 2023). "Long COVID: mechanisms, risk factors and recovery". Experimental Physiology. 108 (1): 12–27. doi:10.1113/EP090802. PMID 36412084. S2CID 253760439.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 Perumal R, Shunmugam L, Naidoo K, Wilkins D, Garzino-Demo A, Brechot C, et al. (June 2023). "Biological mechanisms underpinning the development of long COVID". iScience. 26 (6): 106935. Bibcode:2023iSci...26j6935P. doi:10.1016/j.isci.2023.106935. PMC 10193768. PMID 37265584.
- 1 2 3 Turner S, Khan MA, Putrino D, Woodcock A, Kell DB, Pretorius E (June 2023). "Long COVID: pathophysiological factors and abnormalities of coagulation". Trends in Endocrinology and Metabolism. Pathophysiology of Long COVID. 34 (6): 321–344. doi:10.1016/j.tem.2023.03.002. PMC 10113134. PMID 37080828.
- ↑ Proal AD, VanElzakker MB, Aleman S, Bach K, Boribong BP, Buggert M, et al. (September 2023). "SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC)". Nature Immunology. 24 (10). SARS-CoV-2 reservoir in PASC. doi:10.1038/s41590-023-01601-2. PMID 37667052. S2CID 261527320.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Proal AD, VanElzakker MB, Aleman S, Bach K, Boribong BP, Buggert M, et al. (September 2023). "SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC)". Nature Immunology. 24 (10). Mechanisms of disease. doi:10.1038/s41590-023-01601-2. PMID 37667052. S2CID 261527320.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Chen B, Julg B, Mohandas S, Bradfute SB (May 2023). "Viral persistence, reactivation, and mechanisms of long COVID". eLife. 12. doi:10.7554/eLife.86015. PMC 10159620. PMID 37140960.
- ↑ CDC (2023-07-06). "COVID-19 and Your Health". Centers for Disease Control and Prevention. Retrieved 2023-09-03.
- ↑ Edwards F, Hamilton FW (2023). "Impact of covid-19 vaccination on long covid". BMJ Medicine. 2 (1): e000470. doi:10.1136/bmjmed-2022-000470. PMC 9978666. PMID 36936263.
- ↑ "Review estimates 69% 3-dose vaccine efficacy against long COVID". University of Minnesota. 2023-10-13. Retrieved 2023-10-15.
- ↑ Marra AR, Kobayashi T, Callado GY, Pardo I, Gutfreund MC, Hsieh MK, et al. (2023). "The effectiveness of COVID-19 vaccine in the prevention of post-COVID conditions: a systematic literature review and meta-analysis of the latest research". Antimicrobial Stewardship & Healthcare Epidemiology. 3 (1): e168. doi:10.1017/ash.2023.447. ISSN 2732-494X. PMC 10644173. PMID 38028898. S2CID 263909710.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ "COVID-19 rapid guideline: managing the long-term effects of COVID-19". National Institute for Health and Care Excellence. 2021-11-11. Retrieved 2023-09-09.
- 1 2 3 4 5 6 7 Aiyegbusi OL, Hughes SE, Turner G, Rivera SC, McMullan C, Chandan JS, et al. (September 2021). "Symptoms, complications and management of long COVID: a review". Journal of the Royal Society of Medicine. 114 (9): 428–442. doi:10.1177/01410768211032850. PMC 8450986. PMID 34265229.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 3 4 5 Wolf S, Zechmeister-Koss I, Erdös J (August 2022). "Possible long COVID healthcare pathways: a scoping review". BMC Health Services Research. 22 (1): 1076. doi:10.1186/s12913-022-08384-6. PMC 9396575. PMID 35999605.
- 1 2 3 Ford ND, Slaughter D, Edwards D, Dalton A, Perrine C, Vahratian A, et al. (August 2023). "Long COVID and Significant Activity Limitation Among Adults, by Age – United States, June 1–13, 2022, to June 7–19, 2023". MMWR. Morbidity and Mortality Weekly Report. 72 (32): 866–870. doi:10.15585/mmwr.mm7232a3. PMC 10415000. PMID 37561665.
- ↑ Hastie CE, Lowe DJ, McAuley A, Winter AJ, Mills NL, Black C, et al. (October 2022). "Outcomes among confirmed cases and a matched comparison group in the Long-COVID in Scotland study". Nature Communications. 13 (1): 5663. Bibcode:2022NatCo..13.5663H. doi:10.1038/s41467-022-33415-5. PMC 9556711. PMID 36224173.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Zheng YB, Zeng N, Yuan K, Tian SS, Yang YB, Gao N, et al. (May 2023). "Prevalence and risk factor for long COVID in children and adolescents: A meta-analysis and systematic review". Journal of Infection and Public Health. 16 (5): 660–672. doi:10.1016/j.jiph.2023.03.005. PMC 9990879. PMID 36931142.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Behnood S, Newlands F, O'Mahoney L, Takeda A, Haghighat Ghahfarokhi M, Bennett SD, et al. (2023). "A systematic review and meta-analysis conducted by UCL Great Ormond Street Institute of Child in collaboration with the World Health Organization". A clinical case definition for post covid-19 condition in children and adolescents by expert consensus. World Health Organization. p. 25.
{{cite book}}: CS1 maint: overridden setting (link) - ↑ Jiang L, Li X, Nie J, Tang K, Bhutta ZA (August 2023). "A Systematic Review of Persistent Clinical Features After SARS-CoV-2 in the Pediatric Population". Pediatrics. 152 (2). doi:10.1542/peds.2022-060351. PMC 10389775. PMID 37476923.
- ↑ Messiah SE, Francis J, Weerakoon S, Mathew MS, Shaikh S, Veeraswamy A, et al. (2023-09-21). "Persistent symptoms and conditions among children and adolescents hospitalised with COVID-19 illness: a qualitative study". BMJ Open. 13 (9): e069073. doi:10.1136/bmjopen-2022-069073. PMC 10514629. PMID 37734886.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Rushforth A, Ladds E, Wieringa S, Taylor S, Husain L, Greenhalgh T (October 2021). "Long Covid - The illness narratives". Social Science & Medicine. 286: 114326. doi:10.1016/j.socscimed.2021.114326. hdl:10044/1/91206. PMID 34425522. S2CID 237281271.
- 1 2 Roth PH, Gadebusch-Bondio M (January 2022). "The contested meaning of "long COVID" - Patients, doctors, and the politics of subjective evidence". Social Science & Medicine. 292: 114619. doi:10.1016/j.socscimed.2021.114619. PMC 8629766. PMID 34906823.
- 1 2 3 4 Callard F, Perego E (January 2021). "How and why patients made Long Covid". Social Science & Medicine. 268: 113426. doi:10.1016/j.socscimed.2020.113426. PMC 7539940. PMID 33199035.
- ↑ Witvliet MG (2020-11-27). "Here's how it feels when COVID-19 symptoms last for months". PBS NewsHour. Archived from the original on 2020-11-29. Retrieved 2020-11-29.
- ↑ Macnamara K. "The Covid 'longhaulers' behind a global patient movement". AFP. Archived from the original on 2021-02-04. Retrieved 2021-01-30.
- ↑ "Patient-Led Research Collaborative for Long COVID". Patient Led Research Collaborative. Archived from the original on 2022-01-10. Retrieved 2022-01-08.
- ↑ Callard F, Perego E (January 2021). "How and why patients made Long Covid". Social Science & Medicine. 268: 113426. doi:10.1016/j.socscimed.2020.113426. PMC 7539940. PMID 33199035.
- ↑ Hossain MM, Das J, Rahman F, Nesa F, Hossain P, Islam AM, et al. (2023-02-16). Canzan F (ed.). "Living with "long COVID": A systematic review and meta-synthesis of qualitative evidence". PLOS ONE. 18 (2): e0281884. Bibcode:2023PLoSO..1881884H. doi:10.1371/journal.pone.0281884. PMC 9934341. PMID 36795701.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 Nittas V, Gao M, West EA, Ballouz T, Menges D, Wulf Hanson S, et al. (2022). "Long COVID Through a Public Health Lens: An Umbrella Review". Public Health Reviews. 43: 1604501. doi:10.3389/phrs.2022.1604501. PMC 8963488. PMID 35359614.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Gualano MR, Rossi MF, Borrelli I, Santoro PE, Amantea C, Daniele A, et al. (2022-01-01). "Returning to work and the impact of post COVID-19 condition: A systematic review". Work. 73 (2): 405–413. doi:10.3233/WOR-220103. PMID 35938280. S2CID 251293637.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Waters T, Wernham T (2022). Long COVID and the labour market (PDF). The Institute for Fiscal Studies. pp. 10–11. ISBN 978-1-80103-079-3.
- ↑ "Post-COVID Conditions". Centers for Disease Control and Prevention. 2022-12-16. Retrieved 2023-06-07.
- ↑ Montani D, Savale L, Noel N, Meyrignac O, Colle R, Gasnier M, et al. (March 2022). "Post-acute COVID-19 syndrome". European Respiratory Review. 31 (163): 210185. doi:10.1183/16000617.0185-2021. PMC 8924706. PMID 35264409.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Buonsenso D (2023). "Pharmacological trials for long COVID: first light at the end of the tunnel". The Lancet. Regional Health - Europe. 24: 100544. doi:10.1016/j.lanepe.2022.100544. ISSN 2666-7762. PMC 9647474. PMID 36407125.
- ↑ Subbaraman N (March 2021). "US health agency will invest $1 billion to investigate 'long COVID'". Nature. 591 (7850): 356. Bibcode:2021Natur.591..356S. doi:10.1038/d41586-021-00586-y. PMID 33664445. S2CID 232123730.
- ↑ Cohrs R (2023-07-31). "NIH begins long-delayed clinical trials for long Covid, announces new research office". STAT. Retrieved 2023-07-31.
- ↑ Kozlov M (August 2023). "NIH launches trials for long COVID treatments: what scientists think". Nature. doi:10.1038/d41586-023-02472-1. PMID 37528203. S2CID 260375952.
- 1 2 Walker S, Goodfellow H, Pookarnjanamorakot P, Murray E, Bindman J, Blandford A, et al. (2023-06-01). "Impact of fatigue as the primary determinant of functional limitations among patients with post-COVID-19 syndrome: a cross-sectional observational study". BMJ Open. 13 (6): e069217. doi:10.1136/bmjopen-2022-069217. ISSN 2044-6055. PMC 10335413. PMID 37286327.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ "Long COVID: fatigue predicts poor everyday functioning". UK National Institute for Health and Care Research. 2023-11-23. doi:10.3310/nihrevidence_60359.
Further reading
General
Books
- Jackson JC (2023). Clearing the Fog: From Surviving to Thriving with Long COVID – A Practical Guide. New York: Little, Brown Spark. ISBN 978-0316530095. OCLC 1345215931.
Journal articles
- "Long COVID: let patients help define long-lasting COVID symptoms". Editorial. Nature. 586 (7828): 170. October 2020. Bibcode:2020Natur.586..170.. doi:10.1038/d41586-020-02796-2. PMID 33029005. S2CID 222217022.
- Alwan NA (August 2020). "Track COVID-19 sickness, not just positive tests and deaths". Nature. 584 (7820): 170. doi:10.1038/d41586-020-02335-z. PMID 32782377. S2CID 221107554.
- Kingstone T, Taylor AK, O'Donnell CA, Atherton H, Blane DN, Chew-Graham CA (December 2020). "Finding the 'right' GP: a qualitative study of the experiences of people with long-COVID". BJGP Open. Royal College of General Practitioners. 4 (5): bjgpopen20X101143. doi:10.3399/bjgpopen20X101143. PMC 7880173. PMID 33051223. S2CID 222351478.
- Salisbury H (June 2020). "Helen Salisbury: When will we be well again?". BMJ. 369: m2490. doi:10.1136/bmj.m2490. PMID 32576550. S2CID 219983336.
- "Researching long COVID: addressing a new global health challenge". NIHR Evidence (Plain English summary). 2022-05-12. doi:10.3310/nihrevidence_50331. S2CID 249942230. Archived from the original on 2022-06-25. Retrieved 2022-05-13.
- The Lancet Infectious Diseases (August 2023). "Where are the long COVID trials?". The Lancet. Infectious Diseases. 23 (8): 879. doi:10.1016/S1473-3099(23)00440-1. PMID 37507151. S2CID 260272959.