
An mRNA vaccine is a type of vaccine that uses a copy of a molecule called messenger RNA (mRNA) to produce an immune response.[1] The vaccine delivers molecules of antigen-encoding mRNA into immune cells, which use the designed mRNA as a blueprint to build foreign protein that would normally be produced by a pathogen (such as a virus) or by a cancer cell. These protein molecules stimulate an adaptive immune response that teaches the body to identify and destroy the corresponding pathogen or cancer cells.[1] The mRNA is delivered by a co-formulation of the RNA encapsulated in lipid nanoparticles that protect the RNA strands and help their absorption into the cells.[2][3]
Reactogenicity, the tendency of a vaccine to produce adverse reactions, is similar to that of conventional non-RNA vaccines.[4] People susceptible to an autoimmune response may have an adverse reaction to messenger RNA vaccines.[4] The advantages of mRNA vaccines over traditional vaccines are ease of design, speed and lower cost of production, the induction of both cellular and humoral immunity, and lack of interaction with the genomic DNA.[5][6] While some messenger RNA vaccines, such as the Pfizer–BioNTech COVID-19 vaccine, have the disadvantage of requiring ultracold storage before distribution,[1] other mRNA vaccines, such as the Moderna, CureVac, and Walvax COVID-19 vaccines, do not have such requirements.[7][8]
In RNA therapeutics, messenger RNA vaccines have attracted considerable interest as COVID-19 vaccines.[1] In December 2020, Pfizer–BioNTech and Moderna obtained authorization for their mRNA-based COVID-19 vaccines. On 2 December, the UK Medicines and Healthcare products Regulatory Agency (MHRA) became the first medicines regulator to approve an mRNA vaccine, authorizing the Pfizer–BioNTech vaccine for widespread use.[9][10][11] On 11 December, the US Food and Drug Administration (FDA) issued an emergency use authorization for the Pfizer–BioNTech vaccine[12][13] and a week later similarly authorized the Moderna vaccine.[14][15] The 2023 Nobel Prize in Physiology or Medicine was awarded to Katalin Karikó and Drew Weissman for the development of effective mRNA vaccines against COVID-19.[16][17][18]
History
Early research

The first successful transfection of designed mRNA packaged within a liposomal nanoparticle into a cell was published in 1989.[19][20] "Naked" (or unprotected) lab-made mRNA was injected a year later into the muscle of mice.[3][21] These studies were the first evidence that in vitro transcribed mRNA with a chosen gene was able to deliver the genetic information to produce a desired protein within living cell tissue[3] and led to the concept proposal of messenger RNA vaccines.[22][23][24]
Liposome-encapsulated mRNA encoding a viral antigen was shown in 1993 to stimulate T cells in mice.[25][26] The following year self-amplifying mRNA was developed by including both a viral antigen and replicase encoding gene.[25][27] The method was used in mice to elicit both a humoral and cellular immune response against a viral pathogen.[25] The next year mRNA encoding a tumor antigen was shown to elicit a similar immune response against cancer cells in mice.[28][29]
Development
The first human clinical trial using ex vivo dendritic cells transfected with mRNA encoding tumor antigens (therapeutic cancer mRNA vaccine) was started in 2001.[30][31] Four years later, the successful use of modified nucleosides as a method to transport mRNA inside cells without setting off the body's defense system was reported.[30][32] Clinical trial results of an mRNA vaccine directly injected into the body against cancer cells were reported in 2008.[33][34]
BioNTech in 2008, and Moderna in 2010, were founded to develop mRNA biotechnologies.[35][36] The US research agency DARPA launched at this time the biotechnology research program ADEPT to develop emerging technologies for the US military.[37][38] The agency recognized the potential of nucleic acid technology for defense against pandemics and began to invest in the field.[37] DARPA grants were seen as a vote of confidence that in turn encouraged other government agencies and private investors to invest in mRNA technology.[38] DARPA awarded at the time a $25 million grant to Moderna.[39]
The first human clinical trials using an mRNA vaccine against an infectious agent (rabies) began in 2013.[40][41] Over the next few years, clinical trials of mRNA vaccines for a number of other viruses were started. mRNA vaccines for human use have been studied for infectious agents such as influenza,[42] Zika virus, cytomegalovirus, and Chikungunya virus.[43][44]
In March 2022 Moderna announced the development of mRNA vaccines for 15 diseases: Chikungunya virus, COVID-19, Crimean-Congo haemorrhagic fever, Dengue, Ebola virus disease, HIV, Malaria, Marburg virus disease, Lassa fever, Middle East respiratory syndrome coronavirus (MERS-CoV), Nipah and henipaviral diseases, Rift Valley fever, Severe fever with Thrombocytopenia syndrome, Tuberculosis and Zika.[45][46]
Acceleration
The COVID-19 pandemic, and sequencing of the causative virus SARS-CoV-2 at the beginning of 2020, led to the rapid development of the first approved mRNA vaccines.[47][48] BioNTech and Moderna in December of the same year obtained approval for their mRNA-based COVID-19 vaccines. On 2 December, seven days after its final eight-week trial, the UK Medicines and Healthcare products Regulatory Agency (MHRA) became the first global medicines regulator in history to approve an mRNA vaccine, granting emergency authorization for Pfizer–BioNTech's BNT162b2 COVID-19 vaccine for widespread use.[9][10][49] On 11 December, the FDA gave emergency use authorization for the Pfizer–BioNTech COVID-19 vaccine and a week later similar approval for the Moderna COVID-19 vaccine.[50] Other mRNA vaccines continued under development.
Mechanism
The goal of a vaccine is to stimulate the adaptive immune system to create antibodies that precisely target that particular pathogen. The markers on the pathogen that the antibodies target are called antigens.[51]
Traditional vaccines stimulate an antibody response by injecting either antigens, an attenuated (weakened) virus, an inactivated (dead) virus, or a recombinant antigen-encoding viral vector (harmless carrier virus with an antigen transgene) into the body. These antigens and viruses are prepared and grown outside the body.[52][53]
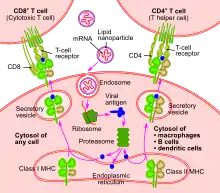
In contrast, mRNA vaccines introduce a short-lived[54] synthetically created fragment of the RNA sequence of a virus into the individual being vaccinated. These mRNA fragments are taken up by dendritic cells through phagocytosis.[55] The dendritic cells use their internal machinery (ribosomes) to read the mRNA and produce the viral antigens that the mRNA encodes.[4] The body degrades the mRNA fragments within a few days of introduction.[56] Although non-immune cells can potentially also absorb vaccine mRNA, produce antigens, and display the antigens on their surfaces, dendritic cells absorb the mRNA globules much more readily.[57] The mRNA fragments are translated in the cytoplasm and do not affect the body's genomic DNA, located separately in the cell nucleus.[1][58]
Once the viral antigens are produced by the host cell, the normal adaptive immune system processes are followed. Antigens are broken down by proteasomes. Class I and class II MHC molecules then attach to the antigen and transport it to the cellular membrane, "activating" the dendritic cell.[58] Once activated, dendritic cells migrate to lymph nodes, where they present the antigen to T cells and B cells.[59] This triggers the production of antibodies specifically targeted to the antigen, ultimately resulting in immunity.[51]
mRNA

The central component of a mRNA vaccine is its mRNA construct.[60] The in vitro transcribed mRNA is generated from an engineered plasmid DNA, which has an RNA polymerase promoter and sequence which corresponds to the mRNA construct. By combining T7 phage RNA polymerase and the plasmid DNA, the mRNA can be transcribed in the lab. Efficacy of the vaccine is dependent on the stability and structure of the designed mRNA.[4]
The in vitro transcribed mRNA has the same structural components as natural mRNA in eukaryotic cells. It has a 5' cap, a 5'-untranslated region (UTR) and 3'-UTR, an open reading frame (ORF), which encodes the relevant antigen, and a 3'-poly(A) tail. By modifying these different components of the synthetic mRNA, the stability and translational ability of the mRNA can be enhanced, and in turn, the efficacy of the vaccine improved.[60]
The mRNA can be improved by using synthetic 5'-cap analogues which enhance the stability and increase protein translation. Similarly, regulatory elements in the 5'-untranslated region and the 3'-untranslated region can be altered, and the length of the poly(A) tail optimized, to stabilize the mRNA and increase protein production. The mRNA nucleotides can be modified to both decrease innate immune activation and increase the mRNA's half-life in the host cell. The nucleic acid sequence and codon usage impacts protein translation. Enriching the sequence with guanine-cytosine content improves mRNA stability and half-life and, in turn, protein production. Replacing rare codons with synonymous codons frequently used by the host cell also enhances protein production.[4]
Delivery

For a vaccine to be successful, sufficient mRNA must enter the host cell cytoplasm to stimulate production of the specific antigens. Entry of mRNA molecules, however, faces a number of difficulties. Not only are mRNA molecules too large to cross the cell membrane by simple diffusion, they are also negatively charged like the cell membrane, which causes a mutual electrostatic repulsion. Additionally, mRNA is easily degraded by RNAases in skin and blood.[58]
Various methods have been developed to overcome these delivery hurdles. The method of vaccine delivery can be broadly classified by whether mRNA transfer into cells occurs within (in vivo) or outside (ex vivo) the organism.[58][3]
Ex vivo
Dendritic cells display antigens on their surfaces, leading to interactions with T cells to initiate an immune response. Dendritic cells can be collected from patients and programmed with the desired mRNA, then administered back into patients to create an immune response.[61]
The simplest way that ex vivo dendritic cells take up mRNA molecules is through endocytosis, a fairly inefficient pathway in the laboratory setting that can be significantly improved through electroporation.[58]
In vivo
Since the discovery that the direct administration of in vitro transcribed mRNA leads to the expression of antigens in the body, in vivo approaches have been investigated.[21] They offer some advantages over ex vivo methods, particularly by avoiding the cost of harvesting and adapting dendritic cells from patients and by imitating a regular infection.[58]
Different routes of injection, such as into the skin, blood, or muscles, result in varying levels of mRNA uptake, making the choice of administration route a critical aspect of in vivo delivery. One study showed, in comparing different routes, that lymph node injection leads to the largest T-cell response.[62]
Naked mRNA injection
Naked mRNA injection means that the delivery of the vaccine is only done in a buffer solution.[63] This mode of mRNA uptake has been known since the 1990s.[21] The first worldwide clinical studies used intradermal injections of naked mRNA for vaccination.[64][65] A variety of methods have been used to deliver naked mRNA, such as subcutaneous, intravenous, and intratumoral injections. Although naked mRNA delivery causes an immune response, the effect is relatively weak, and after injection the mRNA is often rapidly degraded.[58]
Polymer and peptide vectors
Cationic polymers can be mixed with mRNA to generate protective coatings called polyplexes. These protect the recombinant mRNA from ribonucleases and assist its penetration in cells. Protamine is a natural cationic peptide and has been used to encapsulate mRNA for vaccination.[66][67]
Lipid nanoparticle vector

The first time the FDA approved the use of lipid nanoparticles as a drug delivery system was in 2018, when the agency approved the first siRNA drug, Onpattro.[68] Encapsulating the mRNA molecule in lipid nanoparticles was a critical breakthrough for producing viable mRNA vaccines, solving a number of key technical barriers in delivering the mRNA molecule into the host cell.[68][69] Research into using lipids to deliver siRNA to cells became a foundation for similar research into using lipids to deliver mRNA.[70] However, new lipids had to be invented to encapsulate mRNA strands, which are much longer than siRNA strands.[70]
Principally, the lipid provides a layer of protection against degradation, allowing more robust translational output. In addition, the customization of the lipid's outer layer allows the targeting of desired cell types through ligand interactions. However, many studies have also highlighted the difficulty of studying this type of delivery, demonstrating that there is an inconsistency between in vivo and in vitro applications of nanoparticles in terms of cellular intake.[71] The nanoparticles can be administered to the body and transported via multiple routes, such as intravenously or through the lymphatic system.[68]
One issue with lipid nanoparticles is that several of the breakthroughs leading to the practical use of that technology involve the use of microfluidics. Microfluidic reaction chambers are difficult to scale up, since the entire point of microfluidics is to exploit the microscale behaviors of liquids. The only way around this obstacle is to run an extensive number of microfluidic reaction chambers in parallel, a novel task requiring custom-built equipment.[72][73] For COVID-19 mRNA vaccines, this was the main manufacturing bottleneck. Pfizer used such a parallel approach to solve the scaling problem. After verifying that impingement jet mixers could not be directly scaled up,[74] Pfizer made about 100 of the little mixers (each about the size of a U.S. half-dollar coin), connected them together with pumps and filters with a "maze of piping,"[75][76] and set up a computer system to regulate flow and pressure through the mixers.[74]
Another issue, with the large-scale use of this delivery method, is the availability of the novel lipids used to create lipid nanoparticles, especially ionizable cationic lipids. Before 2020, such lipids were manufactured in small quantities measured in grams or kilograms, and they were used for medical research and a handful of drugs for rare conditions. As the safety and efficacy of mRNA vaccines became clear in 2020, the few companies able to manufacture the requisite lipids were confronted with the challenge of scaling up production to respond to orders for several tons of lipids.[73][77]
Viral vector
In addition to non-viral delivery methods, RNA viruses have been engineered to achieve similar immunological responses. Typical RNA viruses used as vectors include retroviruses, lentiviruses, alphaviruses and rhabdoviruses, each of which can differ in structure and function.[78] Clinical studies have utilized such viruses on a range of diseases in model animals such as mice, chicken and primates.[79][80][81]
Advantages
Traditional vaccines

mRNA vaccines offer specific advantages over traditional vaccines.[4][5] Because mRNA vaccines are not constructed from an active pathogen (or even an inactivated pathogen), they are non-infectious. In contrast, traditional vaccines require the production of pathogens, which, if done at high volumes, could increase the risks of localized outbreaks of the virus at the production facility.[5] Another biological advantage of mRNA vaccines is that since the antigens are produced inside the cell, they stimulate cellular immunity, as well as humoral immunity.[6][82]
mRNA vaccines have the production advantage that they can be designed swiftly. Moderna designed their mRNA-1273 vaccine for COVID-19 in 2 days.[83] They can also be manufactured faster, more cheaply, and in a more standardized fashion (with fewer error rates in production), which can improve responsiveness to serious outbreaks.[4][5]
The Pfizer–BioNTech vaccine originally required 110 days to mass-produce (before Pfizer began to optimize the manufacturing process to only 60 days), which was substantially faster than traditional flu and polio vaccines.[75] Within that larger timeframe, the actual production time is only about 22 days: two weeks for molecular cloning of DNA plasmids and purification of DNA, four days for DNA-to-RNA transcription and purification of mRNA, and four days to encapsulate mRNA in lipid nanoparticles followed by fill and finish.[84] The majority of the days needed for each production run are allocated to rigorous quality control at each stage.[75]
DNA vaccines
In addition to sharing the advantages of theoretical DNA vaccines over established traditional vaccines, mRNA vaccines also have additional advantages over DNA vaccines. The mRNA is translated in the cytosol, so there is no need for the RNA to enter the cell nucleus, and the risk of being integrated into the host genome is averted.[3] Modified nucleosides (for example, pseudouridines, 2'-O-methylated nucleosides) can be incorporated to mRNA to suppress immune response stimulation to avoid immediate degradation and produce a more persistent effect through enhanced translation capacity.[32][85][86] The open reading frame (ORF) and untranslated regions (UTR) of mRNA can be optimized for different purposes (a process called sequence engineering of mRNA), for example through enriching the guanine-cytosine content or choosing specific UTRs known to increase translation.[55] An additional ORF coding for a replication mechanism can be added to amplify antigen translation and therefore immune response, decreasing the amount of starting material needed.[87][88]
Disadvantages
Storage
Because mRNA is fragile, some vaccines must be kept at very low temperatures to avoid degrading and thus giving little effective immunity to the recipient. Pfizer–BioNTech's BNT162b2 mRNA vaccine has to be kept between −80 and −60 °C (−112 and −76 °F).[89][90] Moderna says their mRNA-1273 vaccine can be stored between −25 and −15 °C (−13 and 5 °F),[91] which is comparable to a home freezer,[90] and that it remains stable between 2 and 8 °C (36 and 46 °F) for up to 30 days.[91][92] In November 2020, Nature reported, "While it's possible that differences in LNP formulations or mRNA secondary structures could account for the thermostability differences [between Moderna and BioNtech], many experts suspect both vaccine products will ultimately prove to have similar storage requirements and shelf lives under various temperature conditions."[82] Several platforms are being studied that may allow storage at higher temperatures.[4]
Recent
Before 2020, no mRNA technology platform (drug or vaccine) had been authorized for use in humans, so there was a risk of unknown effects.[82] The 2020 COVID-19 pandemic required faster production capability of mRNA vaccines, made them attractive to national health organisations, and led to debate about the type of initial authorization mRNA vaccines should get (including emergency use authorization or expanded access authorization) after the eight-week period of post-final human trials.[93][94]
Side effects
Reactogenicity is similar to that of conventional, non-RNA vaccines. However, those susceptible to an autoimmune response may have an adverse reaction to mRNA vaccines.[4] The mRNA strands in the vaccine may elicit an unintended immune reaction – this entails the body believing itself to be sick, and the person feeling as if they are as a result. To minimize this, mRNA sequences in mRNA vaccines are designed to mimic those produced by host cells.[5]
Strong but transient reactogenic effects were reported in trials of novel COVID-19 mRNA vaccines; most people will not experience severe side effects which include fever and fatigue. Severe side effects are defined as those that prevent daily activity.[95]
Efficacy
The COVID-19 mRNA vaccines from Moderna and Pfizer–BioNTech have efficacy rates of 90 to 95 percent. Prior mRNA, drug trials on pathogens other than COVID-19 were not effective and had to be abandoned in the early phases of trials. The reason for the efficacy of the new mRNA vaccines is not clear.[96]
Physician-scientist Margaret Liu stated that the efficacy of the new COVID-19 mRNA vaccines could be due to the "sheer volume of resources" that went into development, or that the vaccines might be "triggering a nonspecific inflammatory response to the mRNA that could be heightening its specific immune response, given that the modified nucleoside technique reduced inflammation but hasn't eliminated it completely", and that "this may also explain the intense reactions such as aches and fevers reported in some recipients of the mRNA SARS-CoV-2 vaccines". These reactions though severe were transient and another view is that they were believed to be a reaction to the lipid drug delivery molecules.[96]
Hesitancy
There is misinformation implying that mRNA vaccines could alter DNA in the nucleus.[97] mRNA in the cytosol is very rapidly degraded before it would have time to gain entry into the cell nucleus. In fact, mRNA vaccines must be stored at very low temperature and free from RNAses to prevent mRNA degradation. Retrovirus can be single-stranded RNA (just as many SARS-CoV-2 vaccines are single-stranded RNA) which enters the cell nucleus and uses reverse transcriptase to make DNA from the RNA in the cell nucleus. A retrovirus has mechanisms to be imported into the nucleus, but other mRNA (such as the vaccine) lack these mechanisms. Once inside the nucleus, creation of DNA from RNA cannot occur without a reverse transcriptase and appropriate primers, which both accompany a retrovirus, but which would not be present for other exogenous mRNA (such as a vaccine) even if it could enter the nucleus.[98]
Amplification
mRNA vaccines use either non-amplifying (conventional) mRNA or self-amplifying mRNA.[99] Pfizer–BioNTech and Moderna vaccines use non-amplifying mRNA. Both mRNA types continue to be investigated as vaccine methods against other potential pathogens and cancer.[33]
Non-amplifying

The initial mRNA vaccines use a non-amplifying mRNA construct.[67] Non-amplifying mRNA has only one open reading frame that codes for the antigen of interest.[99] The total amount of mRNA available to the cell is equal to the amount delivered by the vaccine. Dosage strength is limited by the amount of mRNA that can be delivered by the vaccine.[100] Non-amplifying vaccines replace uridine with N1-Methylpseudouridine in an attempt to reduce toxicity.[101]
Self-amplifying
Self-amplifying mRNA (saRNA) vaccines replicate their mRNA after transfection.[102] Self-amplifying mRNA has two open reading frames. The first frame, like conventional mRNA, codes for the antigen of interest. The second frame codes for an RNA-dependent RNA polymerase (and its helper proteins) which replicates the mRNA construct in the cell. This allows smaller vaccine doses.[102] The mechanisms and consequently the evaluation of self-amplifying mRNA may be different, as self-amplifying mRNA is a much bigger molecule.[3]
SaRNA vaccines being researched include a malaria vaccine.[103] Gritstone bio started in 2021 a phase 1 trial of an saRNA COVID-19 vaccine, used as a booster vaccine. The vaccine is designed to target both the spike protein of the SARS‑CoV‑2 virus, and viral proteins that may be less prone to genetic variation, to provide greater protection against SARS‑CoV‑2 variants.[104][105] saRNA vaccines must use uridine, which is required for reproduction to occur.[101]
See also
References
- 1 2 3 4 5 Park KS, Sun X, Aikins ME, Moon JJ (December 2020). "Non-viral COVID-19 vaccine delivery systems". Advanced Drug Delivery Reviews. 169: 137–51. doi:10.1016/j.addr.2020.12.008. PMC 7744276. PMID 33340620.
- ↑ Kowalski PS, Rudra A, Miao L, Anderson DG (April 2019). "Delivering the Messenger: Advances in Technologies for Therapeutic mRNA Delivery". Mol Ther. 27 (4): 710–28. doi:10.1016/j.ymthe.2019.02.012. PMC 6453548. PMID 30846391.
- 1 2 3 4 5 6 Verbeke R, Lentacker I, De Smedt SC, Dewitte H (October 2019). "Three decades of messenger RNA vaccine development". Nano Today. 28: 100766. doi:10.1016/j.nantod.2019.100766. hdl:1854/LU-8628303. S2CID 202221207. Archived from the original on 11 January 2021. Retrieved 8 December 2020.
- 1 2 3 4 5 6 7 8 9 Pardi N, Hogan MJ, Porter FW, Weissman D (April 2018). "mRNA vaccines — a new era in vaccinology". Nature Reviews Drug Discovery. 17 (4): 261–279. doi:10.1038/nrd.2017.243. ISSN 1474-1784. PMC 5906799. PMID 29326426.
- 1 2 3 4 5 PHG Foundation (2019). "RNA vaccines: an introduction". University of Cambridge. Archived from the original on 6 December 2018. Retrieved 18 November 2020.
- 1 2 Kramps T, Elders K (2017). "Introduction to RNA Vaccines". RNA Vaccines: Methods and Protocols. Methods in Molecular Biology. Vol. 1499. pp. 1–11. doi:10.1007/978-1-4939-6481-9_1. ISBN 978-1-4939-6479-6. PMID 27987140.
- ↑ Crommelin DJ, Anchordoquy TJ, Volkin DB, Jiskoot W, Mastrobattista E (March 2021). "Addressing the Cold Reality of mRNA Vaccine Stability". Journal of Pharmaceutical Sciences. 110 (3): 997–1001. doi:10.1016/j.xphs.2020.12.006. ISSN 0022-3549. PMC 7834447. PMID 33321139.
- ↑ "Mexico to start late-stage clinical trial for China's mRNA COVID-19 vaccine". Reuters. 11 May 2021. Archived from the original on 23 August 2021. Retrieved 19 August 2021.
- 1 2 "UK authorises Pfizer/BioNTech COVID-19 vaccine" (Press release). Department of Health and Social Care. 2 December 2020. Archived from the original on 2 December 2020. Retrieved 2 December 2020.
- 1 2 Boseley S, Halliday J (2 December 2020). "UK approves Pfizer/BioNTech Covid vaccine for rollout next week". The Guardian. Archived from the original on 2 December 2020. Retrieved 2 December 2020.
- ↑ "Conditions of Authorisation for Pfizer/BioNTech COVID-19 Vaccine" (Decision). Medicines & Healthcare Products Regulatory Agency. 8 December 2020. Archived from the original on 7 December 2020. Retrieved 10 December 2020.
- ↑ "FDA Takes Key Action in Fight Against COVID-19 By Issuing Emergency Use Authorization for First COVID-19 Vaccine". U.S. Food and Drug Administration (FDA) (Press release). 11 December 2020. Archived from the original on 31 January 2021. Retrieved 6 February 2021.
- ↑ Oliver SE, Gargano JW, Marin M, Wallace M, Curran KG, Chamberland M, et al. (December 2020). "The Advisory Committee on Immunization Practices' Interim Recommendation for Use of Pfizer-BioNTech COVID-19 Vaccine – United States, December 2020" (PDF). MMWR Morb Mortal Wkly Rep. 69 (50): 1922–24. doi:10.15585/mmwr.mm6950e2. PMC 7745957. PMID 33332292. Archived (PDF) from the original on 19 December 2020. Retrieved 7 February 2021.
- ↑ "FDA Takes Additional Action in Fight Against COVID-19 By Issuing Emergency Use Authorization for Second COVID-19 Vaccine". U.S. Food and Drug Administration (FDA) (Press release). 18 December 2020. Archived from the original on 19 December 2020. Retrieved 21 December 2020.
- ↑ Oliver SE, Gargano JW, Marin M, Wallace M, Curran KG, Chamberland M, et al. (January 2021). "The Advisory Committee on Immunization Practices' Interim Recommendation for Use of Moderna COVID-19 Vaccine – United States, December 2020" (PDF). MMWR Morb Mortal Wkly Rep. 69 (5152): 1653–56. doi:10.15585/mmwr.mm695152e1. PMC 9191904. PMID 33382675. S2CID 229945697. Archived (PDF) from the original on 9 February 2021. Retrieved 7 February 2021.
- ↑ "The Nobel Prize in Physiology or Medicine 2023". NobelPrize.org. Retrieved 3 October 2023.
- ↑ "Hungarian and US scientists win Nobel for COVID-19 vaccine discoveries". Reuters. 2 October 2023. Retrieved 3 October 2023.
- ↑ "The Nobel Prize in Physiology or Medicine 2023". NobelPrize.org. Retrieved 3 October 2023.
- ↑ Xu S, Yang K, Li R, Zhang L (September 2020). "mRNA Vaccine Era-Mechanisms, Drug Platform and Clinical Prospection". International Journal of Molecular Sciences. 21 (18): 6582. doi:10.3390/ijms21186582. PMC 7554980. PMID 32916818.
Initiation of cationic lipid-mediated mrna transfection; Concept proposal of mRNA-based drugs
- ↑ Malone RW, Felgner PL [in German], Verma IM (August 1989). "Cationic liposome-mediated RNA transfection". Proceedings of the National Academy of Sciences of the United States of America. 86 (16): 6077–81. Bibcode:1989PNAS...86.6077M. doi:10.1073/pnas.86.16.6077. PMC 297778. PMID 2762315.
- 1 2 3 Wolff JA, Malone RW, Williams P, Chong W, Acsadi G, Jani A, Felgner PL [in German] (March 1990). "Direct gene transfer into mouse muscle in vivo". Science. 247 (4949 Pt 1): 1465–8. Bibcode:1990Sci...247.1465W. doi:10.1126/science.1690918. PMID 1690918.
- ↑ May M (31 May 2021). "After COVID-19 successes, researchers push to develop mRNA vaccines for other diseases". Nature. Archived from the original on 13 October 2021. Retrieved 31 July 2021.
When the broad range of vaccines against COVID-19 were being tested in clinical trials, only a few experts expected the unproven technology of mRNA to be the star. Within 10 months, mRNA vaccines were both the first to be approved and the most effective. Although these are the first mRNA vaccines to be approved, the story of mRNA vaccines starts more than 30 years ago, with many bumps in the road along the way. In 1990, the late physician-scientist Jon Wolff and his University of Wisconsin colleagues injected mRNA into mice, which caused cells in the mice to produce the encoded proteins. In many ways, that work served as the first step toward making a vaccine from mRNA, but there was a long way to go—and there still is, for many applications.
- ↑ Xu S, Yang K, Li R, Zhang L (September 2020). "mRNA Vaccine Era-Mechanisms, Drug Platform and Clinical Prospection". International Journal of Molecular Sciences. 21 (18): 6582. doi:10.3390/ijms21186582. PMC 7554980. PMID 32916818.
Concept proposal of mRNA vaccines (1990)
- ↑ Patent: WO1990011092 Archived 14 October 2021 at the Wayback Machine; Inventors: Philip L. Felgner, Jon Asher Wolff, Gary H. Rhodes, Robert Wallace Malone, Dennis A. Carson; Assignees: Vical Inc., Wisconsin Alumni Research Foundation; Title: "Expression of Exogenous Polynucleotide Sequences in a Vertebrate Archived 9 December 2021 at the Wayback Machine"; (Quote: "The present invention relates to introduction of naked DNA and RNA sequences into a vertebrate to achieve controlled expression of a polypeptide. It is useful in gene therapy, vaccination, and any therapeutic situation in which a polypeptide should be administered to cells in vivo"; Example 8: mRNA vaccination of mice to produce the gpl20 protein of HIV virus); Priority date: 21 March 1989; Publication date: 4 October 1990.
- 1 2 3 Pascolo S (August 2004). "Messenger RNA-based vaccines". Expert Opinion on Biological Therapy. 4 (8): 1285–94. doi:10.1517/14712598.4.8.1285. PMID 15268662. S2CID 19350848.
- ↑ Martinon F, Krishnan S, Lenzen G, Magné R, Gomard E, Guillet JG, et al. (July 1993). "Induction of virus-specific cytotoxic T lymphocytes in vivo by liposome-entrapped mRNA". European Journal of Immunology. 23 (7): 1719–22. doi:10.1002/eji.1830230749. PMID 8325342. S2CID 42640967.
- ↑ Zhou X, Berglund P, Rhodes G, Parker SE, Jondal M, Liljeström P (December 1994). "Self-replicating Semliki Forest virus RNA as recombinant vaccine". Vaccine. 12 (16): 1510–14. doi:10.1016/0264-410x(94)90074-4. PMID 7879415.
- ↑ Kallen KJ, Theß A (January 2014). "A development that may evolve into a revolution in medicine: mRNA as the basis for novel, nucleotide-based vaccines and drugs". Therapeutic Advances in Vaccines. 2 (1): 10–31. doi:10.1177/2051013613508729. PMC 3991152. PMID 24757523.
- ↑ Conry RM, LoBuglio AF, Wright M, Sumerel L, Pike MJ, Johanning F, et al. (April 1995). "Characterization of a messenger RNA polynucleotide vaccine vector". Cancer Research. 55 (7): 1397–400. PMID 7882341.
- 1 2 Sahin U, Karikó K, Türeci Ö (October 2014). "mRNA-based therapeutics — developing a new class of drugs". Nature Reviews Drug Discovery. 13 (10): 759–80. doi:10.1038/nrd4278. ISSN 1474-1784. PMID 25233993.
- ↑ Heiser A, Coleman D, Dannull J, Yancey D, Maurice MA, Lallas CD, et al. (February 2002). "Autologous dendritic cells transfected with prostate-specific antigen RNA stimulate CTL responses against metastatic prostate tumors". The Journal of Clinical Investigation. 109 (3): 409–17. doi:10.1172/JCI14364. ISSN 0021-9738. PMC 150859. PMID 11828001.
- 1 2 Karikó K, Buckstein M, Ni H, Weissman D (August 2005). "Suppression of RNA recognition by Toll-like receptors: the impact of nucleoside modification and the evolutionary origin of RNA". Immunity. 23 (2): 165–75. doi:10.1016/j.immuni.2005.06.008. PMID 16111635.
- 1 2 Blakney AK, Ip S, Geall AJ (January 2021). "An Update on Self-Amplifying mRNA Vaccine Development". Vaccines. 9 (2): 97. doi:10.3390/vaccines9020097. PMC 7911542. PMID 33525396.
- ↑ Weide B, Carralot JP, Reese A, Scheel B, Eigentler TK, Hoerr I, et al. (February–March 2008). "Results of the first phase I/II clinical vaccination trial with direct injection of mRNA". Journal of Immunotherapy. 31 (2): 180–8. doi:10.1097/CJI.0b013e31815ce501. PMID 18481387. S2CID 8233422.
- ↑ "BioNTech's founders: scientist couple in global spotlight". France 24. 13 November 2020. Archived from the original on 14 February 2021. Retrieved 31 July 2021.
- ↑ Garade D (10 November 2020). "The story of mRNA: How a once-dismissed idea became a leading technology in the Covid vaccine race". Stat. Archived from the original on 10 November 2020. Retrieved 16 November 2020.
- 1 2 Sonne P (30 July 2020). "How a secretive Pentagon agency seeded the ground for a rapid coronavirus cure". The Washington Post. Archived from the original on 2 August 2021. Retrieved 21 June 2021.
- 1 2 Usdin S (19 March 2020). "DARPA's gambles might have created the best hopes for stopping COVID-19". BioCentury. Archived from the original on 18 June 2021. Retrieved 19 June 2021.
- ↑ "DARPA Awards Moderna Therapeutics A Grant For Up To $25 Million To Develop Messenger RNA Therapeutics" (Press release). 2 October 2013. Archived from the original on 2 June 2021. Retrieved 31 May 2021.
- ↑ Dolgin E (September 2021). "The tangled history of mRNA vaccines". Nature. 597 (7876): 318–24. Bibcode:2021Natur.597..318D. doi:10.1038/d41586-021-02483-w. ISSN 0028-0836. PMID 34522017. S2CID 237515383.
- ↑ Alberer M, Gnad-Vogt U, Hong HS, Mehr KT, Backert L, Finak G, et al. (September 2017). "Safety and immunogenicity of a mRNA rabies vaccine in healthy adults: an open-label, non-randomised, prospective, first-in-human phase 1 clinical trial". The Lancet. 390 (10101): 1511–20. doi:10.1016/S0140-6736(17)31665-3. PMID 28754494. S2CID 7700297.
- ↑ Dolgin E (November 2021). "mRNA flu shots move into trials". Nature Reviews Drug Discovery. 20 (11): 801–3. doi:10.1038/d41573-021-00176-7. PMID 34635829. S2CID 238637957.
- ↑ Hou X, Zaks T, Langer R, Dong Y (August 2021). "Lipid nanoparticles for mRNA delivery". Nature Reviews Materials. 6 (12): 1078–94. Bibcode:2021NatRM...6.1078H. doi:10.1038/s41578-021-00358-0. ISSN 2058-8437. PMC 8353930. PMID 34394960.
- ↑ "COVID-19 and Your Health". Centers for Disease Control and Prevention. 11 February 2020. Archived from the original on 3 March 2021. Retrieved 26 November 2020.
- ↑ "Moderna Announces Its Global Public Health Strategy". investors.modernatx.com. Archived from the original on 16 March 2022. Retrieved 15 March 2022.
- ↑ Steenhuysen, Julie; Erman, Michael (8 March 2022). "Moderna plots vaccines against 15 pathogens with future pandemic potential". Reuters. Archived from the original on 14 March 2022. Retrieved 15 March 2022.
- ↑ Ball P (January 2021). "The lightning-fast quest for COVID vaccines — and what it means for other diseases". Nature. 589 (7840): 16–18. Bibcode:2021Natur.589...16B. doi:10.1038/d41586-020-03626-1. PMID 33340018. S2CID 229324351.
- ↑ Wherry EJ, Jaffee EM, Warren N, D'Souza G, Ribas A (April 2021). "How Did We Get a COVID-19 Vaccine in Less Than 1 Year?". Clinical Cancer Research. 27 (8): 2136–38. doi:10.1158/1078-0432.CCR-21-0079. ISSN 1078-0432. PMC 8052930. PMID 33542081.
- ↑ Roberts M (2 December 2020). "Covid Pfizer vaccine approved for use next week in UK". BBC News. Archived from the original on 2 December 2020. Retrieved 2 December 2020.
- ↑ Office of the Commissioner (18 December 2020). "Pfizer-BioNTech COVID-19 Vaccine". FDA. Archived from the original on 14 January 2021. Retrieved 21 December 2020.
- 1 2 Batty CJ, Heise MT, Bachelder EM, Ainslie KM (December 2020). "Vaccine formulations in clinical development for the prevention of severe acute respiratory syndrome coronavirus 2 infection". Advanced Drug Delivery Reviews. 169: 168–89. doi:10.1016/j.addr.2020.12.006. PMC 7733686. PMID 33316346.
- ↑ Kyriakidis NC, López-Cortés A, González EV, Grimaldos AB, Prado EO (February 2021). "SARS-CoV-2 vaccines strategies: a comprehensive review of phase 3 candidates". npj Vaccines. 6 (1): 28. doi:10.1038/s41541-021-00292-w. PMC 7900244. PMID 33619260.
- ↑ Bull JJ, Nuismer SL, Antia R (July 2019). "Recombinant vector vaccine evolution". PLOS Computational Biology. 15 (7): e1006857. Bibcode:2019PLSCB..15E6857B. doi:10.1371/journal.pcbi.1006857. PMC 6668849. PMID 31323032.
- ↑ Hajj KA, Whitehead KA (September 2017). "Tools for translation: non-viral materials for therapeutic mRNA delivery". Nature Reviews Materials. 2 (10): 17056. Bibcode:2017NatRM...217056H. doi:10.1038/natrevmats.2017.56.
- 1 2 Schlake T, Thess A, Fotin-Mleczek M, Kallen KJ (November 2012). "Developing mRNA-vaccine technologies". RNA Biology. 9 (11): 1319–30. doi:10.4161/rna.22269. PMC 3597572. PMID 23064118.
- ↑ Anand P, Stahel VP (May 2021). "Review the safety of Covid-19 mRNA vaccines: a review". Patient Safety in Surgery. 15 (1): 20. doi:10.1186/s13037-021-00291-9. PMC 8087878. PMID 33933145.
- ↑ Goldman B (22 December 2020). "How do the new COVID-19 vaccines work?". Scope. Stanford Medicine. Archived from the original on 30 January 2021. Retrieved 28 January 2021.
- 1 2 3 4 5 6 7 Xu S, Yang K, Li R, Zhang L (September 2020). "mRNA Vaccine Era—Mechanisms, Drug Platform and Clinical Prospection". International Journal of Molecular Sciences. 21 (18): 6582. doi:10.3390/ijms21186582. PMC 7554980. PMID 32916818.
- ↑ Fiedler K, Lazzaro S, Lutz J, Rauch S, Heidenreich R (2016). "MRNA Cancer Vaccines". Current Strategies in Cancer Gene Therapy. Recent Results in Cancer Research. Vol. 209. pp. 61–85. doi:10.1007/978-3-319-42934-2_5. ISBN 978-3-319-42932-8. PMID 28101688.
{{cite book}}:|journal=ignored (help) - 1 2 Jackson NA, Kester KE, Casimiro D, Gurunathan S, DeRosa F (February 2020). "The promise of mRNA vaccines: a biotech and industrial perspective". npj Vaccines. 5 (1): 11. doi:10.1038/s41541-020-0159-8. ISSN 2059-0105. PMC 7000814. PMID 32047656.
- ↑ Benteyn D, Heirman C, Bonehill A, Thielemans K, Breckpot K (February 2015). "mRNA-based dendritic cell vaccines". Expert Review of Vaccines. 14 (2): 161–76. doi:10.1586/14760584.2014.957684. PMID 25196947. S2CID 38292712.
- ↑ Kreiter S, Selmi A, Diken M, Koslowski M, Britten CM, Huber C, et al. (November 2010). "Intranodal vaccination with naked antigen-encoding RNA elicits potent prophylactic and therapeutic antitumoral immunity". Cancer Research. 70 (22): 9031–40. doi:10.1158/0008-5472.can-10-0699. PMID 21045153.
- ↑ "Vaccine components". Immunisation Advisory Centre. 22 September 2016. Archived from the original on 26 January 2021. Retrieved 20 December 2020.
- ↑ Probst J, Weide B, Scheel B, Pichler BJ, Hoerr I, Rammensee HG, Pascolo S (August 2007). "Spontaneous cellular uptake of exogenous messenger RNA in vivo is nucleic acid-specific, saturable and ion dependent". Gene Therapy. 14 (15): 1175–80. doi:10.1038/sj.gt.3302964. PMID 17476302.
- ↑ Lorenz C, Fotin-Mleczek M, Roth G, Becker C, Dam TC, Verdurmen WP, et al. (July 2011). "Protein expression from exogenous mRNA: uptake by receptor-mediated endocytosis and trafficking via the lysosomal pathway". RNA Biology. 8 (4): 627–36. doi:10.4161/rna.8.4.15394. PMID 21654214.
- ↑ Weide B, Pascolo S, Scheel B, Derhovanessian E, Pflugfelder A, Eigentler TK, et al. (June 2009). "Direct injection of protamine-protected mRNA: results of a phase 1/2 vaccination trial in metastatic melanoma patients". Journal of Immunotherapy. 32 (5): 498–507. doi:10.1097/CJI.0b013e3181a00068. PMID 19609242. S2CID 3278811.
- 1 2 Wang Y, Zhang Z, Luo J, Han X, Wei Y, Wei X (February 2021). "mRNA vaccine: a potential therapeutic strategy". Molecular Cancer. 20 (1): 33. doi:10.1186/s12943-021-01311-z. PMC 7884263. PMID 33593376.
- 1 2 3 Cooney E (1 December 2020). "How nanotechnology helps mRNA Covid-19 vaccines work". Stat. Archived from the original on 1 December 2020. Retrieved 3 December 2020.
- ↑ Reichmuth AM, Oberli MA, Jaklenec A, Langer R, Blankschtein D (May 2016). "mRNA vaccine delivery using lipid nanoparticles". Therapeutic Delivery. 7 (5): 319–34. doi:10.4155/tde-2016-0006. PMC 5439223. PMID 27075952.
- 1 2 Cross R (6 March 2021). "Without these lipid shells, there would be no mRNA vaccines for COVID-19". Chemical & Engineering News. American Chemical Society. Archived from the original on 5 March 2021. Retrieved 6 March 2021.
- ↑ Paunovska K, Sago CD, Monaco CM, Hudson WH, Castro MG, Rudoltz TG, et al. (March 2018). "A Direct Comparison of in Vitro and in Vivo Nucleic Acid Delivery Mediated by Hundreds of Nanoparticles Reveals a Weak Correlation". Nano Letters. 18 (3): 2148–57. Bibcode:2018NanoL..18.2148P. doi:10.1021/acs.nanolett.8b00432. PMC 6054134. PMID 29489381.
- ↑ Lowe D (3 February 2021). "Opinion: A straightforward explanation why more COVID-19 vaccines can't be produced with help from 'dozens' of companies". MarketWatch. Archived from the original on 5 February 2021. Retrieved 5 February 2021.
- 1 2 King A (23 March 2021). "Why manufacturing Covid vaccines at scale is hard". Chemistry World. Royal Society of Chemistry. Archived from the original on 24 March 2021. Retrieved 26 March 2021.
- 1 2 Sealy A (2 April 2021). "Manufacturing moonshot: How Pfizer makes its millions of Covid-19 vaccine doses". CNN. Archived from the original on 1 April 2021. Retrieved 3 April 2021.
- 1 2 3 Weise E, Weintraub K (7 February 2021). "Race to the Vaccine: A COVID-19 vaccine life cycle: from DNA to doses". USA Today. Gannett. Archived from the original on 25 February 2021. Retrieved 24 February 2021.
- ↑ Hopkins JS, Eastwood J, Moriarty D (3 March 2021). "mRNA Covid-19 Vaccines Are Fast to Make, but Hard to Scale". The Wall Street Journal. Archived from the original on 4 April 2021. Retrieved 3 April 2021.
- ↑ Rowland C (18 February 2021). "Why grandparents can't find vaccines: Scarcity of niche biotech ingredients". The Washington Post. Archived from the original on 26 February 2021. Retrieved 7 March 2021.
- ↑ Lundstrom K (March 2019). "RNA Viruses as Tools in Gene Therapy and Vaccine Development". Genes. 10 (3): 189. doi:10.3390/genes10030189. PMC 6471356. PMID 30832256.
- ↑ Huang TT, Parab S, Burnett R, Diago O, Ostertag D, Hofman FM, et al. (February 2015). "Intravenous administration of retroviral replicating vector, Toca 511, demonstrates therapeutic efficacy in orthotopic immune-competent mouse glioma model". Human Gene Therapy. 26 (2): 82–93. doi:10.1089/hum.2014.100. PMC 4326030. PMID 25419577.
- ↑ Schultz-Cherry S, Dybing JK, Davis NL, Williamson C, Suarez DL, Johnston R, Perdue ML (December 2000). "Influenza virus (A/HK/156/97) hemagglutinin expressed by an alphavirus replicon system protects chickens against lethal infection with Hong Kong-origin H5N1 viruses". Virology. 278 (1): 55–59. doi:10.1006/viro.2000.0635. PMID 11112481.
- ↑ Geisbert TW, Feldmann H (November 2011). "Recombinant vesicular stomatitis virus-based vaccines against Ebola and Marburg virus infections". The Journal of Infectious Diseases. 204 (Suppl 3): S1075–81. doi:10.1093/infdis/jir349. PMC 3218670. PMID 21987744.
- 1 2 3 Dolgin E (November 2020). "COVID-19 vaccines poised for launch, but impact on pandemic unclear". Nature Biotechnology. doi:10.1038/d41587-020-00022-y. PMID 33239758. S2CID 227176634.
- ↑ Neilson S, Dunn A, Bendix A (26 November 2020). "Moderna's groundbreaking coronavirus vaccine was designed in just 2 days". Business Insider. Archived from the original on 11 January 2021. Retrieved 28 November 2020.
- ↑ Rabson M (27 February 2021). "From science to syringe: COVID-19 vaccines are miracles of science and supply chains". CTV News. Bell Media. Archived from the original on 27 February 2021. Retrieved 28 February 2021.
- ↑ Karikó K, Muramatsu H, Ludwig J, Weissman D (November 2011). "Generating the optimal mRNA for therapy: HPLC purification eliminates immune activation and improves translation of nucleoside-modified, protein-encoding mRNA". Nucleic Acids Research. 39 (21): e142. doi:10.1093/nar/gkr695. PMC 3241667. PMID 21890902.
- ↑ Pardi N, Weissman D (17 December 2016). "Nucleoside Modified mRNA Vaccines for Infectious Diseases". RNA Vaccines. Methods in Molecular Biology. Vol. 1499. Springer New York. pp. 109–21. doi:10.1007/978-1-4939-6481-9_6. ISBN 978-1-4939-6479-6. PMID 27987145.
- ↑ Berglund P, Smerdou C, Fleeton MN, Tubulekas I, Liljeström P (June 1998). "Enhancing immune responses using suicidal DNA vaccines". Nature Biotechnology. 16 (6): 562–65. doi:10.1038/nbt0698-562. PMID 9624688. S2CID 38532700.
- ↑ Vogel AB, Lambert L, Kinnear E, Busse D, Erbar S, Reuter KC, et al. (February 2018). "Self-Amplifying RNA Vaccines Give Equivalent Protection against Influenza to mRNA Vaccines but at Much Lower Doses". Molecular Therapy. 26 (2): 446–55. doi:10.1016/j.ymthe.2017.11.017. PMC 5835025. PMID 29275847.
- ↑ "Pfizer-BioNTech COVID-19 Vaccine Vaccination Storage & Dry Ice Safety Handling". Pfizer. Archived from the original on 24 January 2021. Retrieved 17 December 2020.
- 1 2 Simmons-Duffin S. "Why Does Pfizer's COVID-19 Vaccine Need To Be Kept Colder Than Antarctica?". NPR.org. Archived from the original on 1 February 2021. Retrieved 18 November 2020.
- 1 2 "Fact Sheet for Healthcare Providers Administering Vaccine" (PDF). ModernaTX, Inc. Archived from the original on 28 January 2021. Retrieved 21 December 2020.
- ↑ "Moderna Announces Longer Shelf Life for its COVID-19 Vaccine Candidate at Refrigerated Temperatures". NPR.org. Archived from the original on 16 November 2020. Retrieved 18 November 2020.
- ↑ Thomas K (22 October 2020). "Experts Tell F.D.A. It Should Gather More Safety Data on Covid-19 Vaccines". New York Times. Archived from the original on 26 January 2021. Retrieved 21 November 2020.
- ↑ Kuchler H (30 September 2020). "Pfizer boss warns on risk of fast-tracking vaccines". Financial Times. Archived from the original on 18 November 2020. Retrieved 21 November 2020.
- ↑ Wadman M (November 2020). "Public needs to prep for vaccine side effects". Science. 370 (6520): 1022. doi:10.1126/science.370.6520.1022. PMID 33243869.
- 1 2 Kwon D (25 November 2020). "The Promise of mRNA Vaccines". The Scientist. Archived from the original on 22 January 2021. Retrieved 27 November 2020.
- ↑ Carmichael F, Goodman J (2 December 2020). "Vaccine rumours debunked: Microchips, 'altered DNA' and more" (Reality Check). BBC. Archived from the original on 13 March 2021. Retrieved 10 December 2020.
- ↑ Skalka AM (2014). "Retroviral DNA Transposition: Themes and Variations". Microbiology Spectrum. 2 (5): 1101–23. doi:10.1128/microbiolspec.MDNA3-0005-2014. ISBN 9781555819200. PMC 4383315. PMID 25844274.
- 1 2 Deering RP, Kommareddy S, Ulmer JB, Brito LA, Geall AJ (June 2014). "Nucleic acid vaccines: prospects for non-viral delivery of mRNA vaccines". Expert Opin Drug Deliv. 11 (6): 885–99. doi:10.1517/17425247.2014.901308. PMID 24665982. S2CID 33489182.
- ↑ Versteeg L, Almutairi MM, Hotez PJ, Pollet J (September 2019). "Enlisting the mRNA Vaccine Platform to Combat Parasitic Infections". Vaccines. 7 (4): 122. doi:10.3390/vaccines7040122. PMC 6963228. PMID 31547081.
- 1 2 "New crop of COVID-19 mRNA vaccines could be easier to store, cheaper to use". www.science.org. Archived from the original on 5 April 2022. Retrieved 6 April 2022.
- 1 2 Bloom K, van den Berg F, Arbuthnot P (April 2021). "Self-amplifying RNA vaccines for infectious diseases". Gene Therapy. 28 (3–4): 117–129. doi:10.1038/s41434-020-00204-y. PMC 7580817. PMID 33093657.
- ↑ Lowe D (1 March 2021). "A Malaria Vaccine Candidate". Science Translational Medicine. Archived from the original on 6 May 2021. Retrieved 7 May 2021.
- ↑ Knapton, Sarah (20 September 2021). "First 'variant-proof' Covid vaccine starts trials in Manchester - Retired couple Andrew Clarke, 63, and his wife Helen, 64, from Bolton, became the first to receive the mRNA vaccine on Monday". The Daily Telegraph. Archived from the original on 20 September 2021. Retrieved 21 September 2021.
- ↑ "Gritstone Announces Dosing of First Volunteer in Trial Evaluating Self-Amplifying mRNA as a COVID-19 Vaccine Booster and Immunogenicity Enhancer". PipelineReview. 20 September 2021. Archived from the original on 22 September 2021. Retrieved 21 September 2021.
Further reading
- Dolgin E (September 2021). "The tangled history of mRNA vaccines" (PDF). Nature. 597 (9): 318–24. Bibcode:2021Natur.597..318D. doi:10.1038/d41586-021-02483-w. PMID 34522017. S2CID 237515383.
- Sahin U, Karikó K, Türeci Ö (October 2014). "mRNA-based therapeutics – developing a new class of drugs". Nat Rev Drug Discov. 13 (10): 759–80. doi:10.1038/nrd4278. PMID 25233993.
External links
- "Five things you need to know about: mRNA vaccines". Horizon. Archived from the original on 4 April 2020. Retrieved 17 November 2020.
- "RNA vaccines: an introduction". PHG Foundation. University of Cambridge.
- "Understanding mRNA COVID-19 Vaccines". Centers for Disease Control and Prevention. 4 January 2022.
- Kolata, Gina; Mueller, Benjamin (15 January 2022). "Halting Progress and Happy Accidents: How mRNA Vaccines Were Made". The New York Times.
- M.I.T. Lecture 10: Kizzmekia Corbett, Vaccines" on YouTube
- xkcd webcomic explaining how the vaccine works using Star Wars characters and situations.